
WHAT IF ALL DISEASES WERE THE RESULT OF SCAR TISSUE? MORE ON THE FASCIA, ECM, INFLAMMATION, FIBROSIS, MORTALITY, CONNECTION
For at least two decades I’ve been educating my patients about the root causes of sickness and disease. In fact, the more I study this issue, the more I realize that when you boil it all down, different sicknesses and diseases could mostly be thought of as slightly different variations of the same aberrant physiological pathways (HERE), all of which lead to something called FIBROSIS — the number one cause of death in the United States of America (HERE). For instance….
A study in a 2012 issue of the British Journal of Pharmacology summed this up nicely. “Fibrosis, the result of excess deposition of extracellular matrix (ECM), in particular collagen, leads to scarring and loss of function in tissues that include the heart, lung, kidney and liver.” In other words, excess ECM leads not only to thickening of tissues (including connective tissues) via a process known as “DENSIFICATION,” but causes the same sort of thickening and increased density in other tissues as well.
Unfortunately, excess tissue density leads to poor cellular function, making it simple to understand why the organs mentioned above are affected. Although I’ve written about this phenomenon on several occasions, allow me to lead you through the progression systematically, showing you that while all roads might lead to Rome, most diseases are ultimately the result of inflammation and fibrosis.
I’ve shown you time and time again that most diseases have common origins, but take a look at the abstract of the massively-bibbled review (Extracellular Matrix Degradation and Remodeling in Development and Disease) from the journal, Perspectives in Biology.
The extracellular matrix (ECM) serves diverse functions and is a major component of the cellular microenvironment. The ECM is a highly dynamic structure, constantly undergoing a remodeling process where ECM components are deposited, degraded, or otherwise modified.
ECM dynamics are indispensible during restructuring of tissue architecture. ECM remodeling is an important mechanism whereby cell differentiation can be regulated, including processes such as the establishment and maintenance of stem cell niches, branching morphogenesis, angiogenesis, bone remodeling, and wound repair. In contrast, abnormal ECM dynamics lead to deregulated cell proliferation and invasion, failure of cell death, and loss of cell differentiation, resulting in congenital defects and pathological processes including tissue fibrosis and cancer.
Although it’s somewhat shocking, it’s what you find time and time again with almost any disease you care to look at. Take, for instance, Diabesity (the common combination of DIABETES & OBESITY). Just last year, Immuno-Targets and Therapy (The Role of Adipokines in Chronic Inflammation) said something I’ve shared with you in the past — that adipose tissue (body fat) is not inert; it’s an endocrine organ (HERE). The study went on to talk about the fact that adipokines are analogous to CYTOKINES (cellular messengers that both affect and are affected by inflammation).
What drives the adipokines to an inflammatory state? It’s easy enough to deduce after seeing that the chief method described by these authors of reversing this “chronic low-grade state of inflammation and metabolic disorder” was “calorie restriction and starvation“. Since starvation is not an option (at least for the long term), the easiest way to get the body to mimic it’s metabolic effects is via a KETOGENIC DIET.
Another major problem associated with obesity is hypoxia — tissue being starved for OXYGEN. A study from the November 2016 issue of Biochemical Pharmacology (Adipose Extracellular Matrix Remodelling in Obesity and Insulin Resistance) stated that, “It is well understood that a hypoxic response is observed in adipose tissue expansion during obesity progression and that hypoxic response accelerates fibrosis and inflammation. The expansion of adipose tissues should require angiogenesis; however, the excess deposition of ECM limits the angiogenic response of white adipose tissues in obesity.”
In other words, hypoxia causes fibrosis, and fibrosis limits the body’s ability to create new blood vessels. The authors concluded that this mess results in “fibrosis, excess deposition of ECM components, in metabolically active, insulin-sensitive tissues, including the skeletal muscle, adipose tissue and liver, has damaging impact on glucose homoeostasis,” which is ultimately what leads to INSULIN RESISTANCE.
A study from a 2015 issue of Science Translational Medicine says it all in its title — Obesity-Dependent Changes in Interstitial ECM Mechanics Promote Breast Tumorigenesis. As you might suspect, the authors (all twenty of them, from Cornell and Sloan Kettering) concluded that, “obesity-induced interstitial fibrosis promotes breast tumorigenesis by altering mammary ECM mechanics.” The last phrase (altered ECM mechanics) is talking about fibrosis / SCAR TISSUE / densification — whatever you choose to call it.
In another study; this from Vascular Health and Risk Management on kidneys, the authors concluded that in diabetics, “over time… chronic hyperglycemia can cause tissue injury. One pathological response to tissue injury is the development of fibrosis, which involves predominant extracellular matrix (ECM) accumulation.” What’s interesting is that the authors found numerous urinary markers showing this, most of which would be classified as “INFLAMMATION“.
Sugar is funky stuff because it is not only one of the single most inflammatory things you can put in your body (HERE), it can be brutally ADDICTIVE and feed a host of nasties, including INFECTION (dysbiosis is a form of infection). Listen to this email I got from Djordje Stojk of Norway yesterday.
“Quick question after seeing your article on sugar and the immune system. This summer, me and my cousin went to vacation to Greece, and there both of us developed some sort of ear infection along with slight ringing. Doctors say it will pass once the fluid from the infection clears away, but that it may take a year. Anyway, what I’ve noticed, is that when I eat a lot of sugar, it gets very annoyingly loud, and when I cut down on the sugar, it’s barely noticeable at all. Do you think this is coincidence, or can sugar really have this effect?”
Heck no it’s not a coincidence! The inflammatory nature of sugar (and high glycemic carbs) is possibly the biggest of many keys that will open Pandora’s Box, where who-knows-what might be lurking inside, including tendon problems.
Two different studies showed this by revealing how science is attempting to treat these common problems. In the first (Single Dose of Inducible Nitric Oxide Synthase Inhibitor Induces Prolonged Inflammatory Cell Accumulation and Fibrosis Around Injured Tendon and Synovium from an old issue of Mediators of Inflammation); when the powerful FREE RADICAL NO (nitric oxide) was inhibited, tendons failed to heal properly (“NO regulates wound healing and that inhibition of NO synthesis may be directly related to impaired healing of wounds.“).
In another study — this one from last month’s issue of Oncotarget (Metformin Prevents Peritendinous Fibrosis by Inhibiting Transforming Growth Factor-β Signaling) the most common diabetes drug was used to halt tendon fibrosis (TENDINOSIS). As a side note, our national sugar consumption is so out of control that metformin is now being used as a primary treatment for TYPE III DIABETES (Alzheimer’s), as well as PCOS.
Although the Reactive Oxygen Species in the case above, was a necessary component of healing, for the most part, ROS / Free Radicals are a detriment. A decade ago, the American Journal of Pathology (Oral Glycotoxins Determine the Effects of Calorie Restriction on Oxidant Stress, Age-Related Diseases, and Lifespan) showed how AGES (Advanced Glycation Endproducts) kill via OXIDATIVE STRESS-INDUCED Scar Tissue formation, causing “insulin resistance, marked myocardial and renal fibrosis, and shortened lifespan.”
Two years ago Redox Biology concluded that the whole process causes the whole process. “Transforming growth factor beta (TGF-β) is the most potent pro-fibrogenic cytokine and its expression is increased in almost all of fibrotic diseases. TGF-β1 increases ROS production and suppresses antioxidant enzymes, leading to a redox imbalance. ROS, in turn, induce/activate TGF-β1 and mediate many of TGF-β’s fibrogenic effects, forming a vicious cycle.” How do you stop this cycle?
This month’s issue of the Journal of Diabetes & Metabolic Disorders provides the answer via it’s title…. Carbohydrate Restriction Ameliorates Nephropathy by Reducing Oxidative Stress. From what I’ve shown you, we could just as well substitute the word “Fibrosis” for the word “nephropathy”.
Because I have so much information about Scar Tissue on my site (HERE), I routinely get emails asking about “adhesions” — either of the female sort as seen in ENDOMETRIOSIS, or POST-SURGICALLY. This past summer, Disease Models and Mechanisms carried an Austrian study that excited its authors because for the first time they could experimentally mimic the conditions that cause post-surgical adhesions. Why were they so excited about this?
Because in their quest for the next big drug, they now have the ability to induce Scar Tissue / Fibrosis in as many test animals as they desire. Their conclusions mimic the warning I give my patients who are preparing to undergo surgery — go into it as uninflamed as is humanly possible. “Inflammation, fibrosis and perineural adhesions with the surrounding tissue [nerves sticking to tissue — horrendously painful] are common pathological processes following nerve injury and surgical interventions on peripheral nerves in human patients.”
This is why nerve entrapment-release surgeries can be so risky, as well as why there are less invasive methods one may want to try first (HERE). Let’s shift gears for a moment and talk about another potential driver of inflammation — gluten.
 |
One way we can determine how severe your body is reacting against gluten is to look at antibodies, with one of the more common tests being the Anti-Tissue Transglutaminase Test. Tissue Transglutaminase (TG2 or tTG) is an enzyme (suffixes of “ase” denote this), which, according to a study from the International Review of Cell and Molecular Biology (Cellular Functions of Tissue Transglutaminase) is responsible for many important functions.
“A vast array of biochemical activities of TG2 accounts for its involvement in a variety of cellular processes, including adhesion, migration, growth, survival, apoptosis [pre-programmed cell death], differentiation, and extracellular matrix organization [ECM]. In turn, the impact of TG2 on these processes implicates this protein in various physiological responses and pathological states, contributing to wound healing, inflammation, autoimmunity, neurodegeneration, vascular remodeling, tumor growth and metastasis, and tissue fibrosis.”
In case you didn’t get that, reread it until you do.
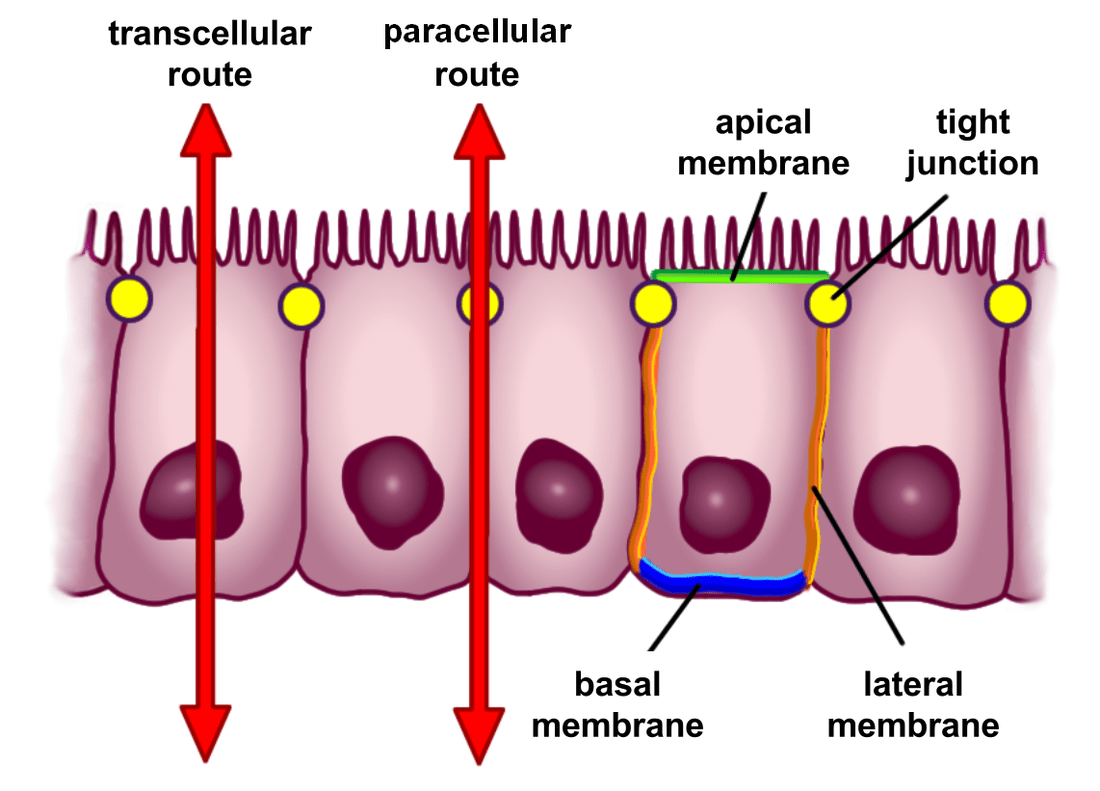
This information is critical once you grasp that TG2 is the auto-antigen (the substance that’s being attacked in autoimmune fashion) by those with CELIAC DISEASE, resulting in atrophy of the villi / microvilli (HERE). The process is driven by inflammatory reactions against gluten, and also affects the tight junctions (see pic above). When the tight junctions become loose, your body starts allowing things into the blood stream (undigested food particles, bacterial or parasite fragments, and others) that should not be there (see previous link).
The body further ramps up it’s immune response because it sees these entities as invaders, subsequently attacking them. Be aware that this process (the “LEAKY GUT“) will often proceed the autoimmunity but can be caused by autoimmunity as well (HERE). To reiterate the seriousness of this viscous cycle, listen to the authors of a study published in the Journal of Biological Chemistry (Characterization of Heparin-Binding Site of Tissue Transglutaminase) discussing some of the craziness that happens when this system breaks down.
“Overexpression of tissue transglutaminase (TG2) is closely related to a wide range of pathological processes, such as wound healing and scarring, fibrosis, celiac disease, multiple sclerosis, and tumor metastasis. Under stress, cells over-express TG2, leading to enhanced externalization of the enzyme and the increased deposition of TG2 into the extracellular matrix (ECM).”
MECHANOTRANSDUCTION is the process of turning a mechanical stimuli into electrical impulses (it’s essentially how the body creates it’s own electricity). A number of years ago, a group of researchers working out of Cal State S.F.’s Lab published a study in Nature Reviews Molecular Cell Biology called Balancing Forces: Architectural Control of Mechanotransduction. Pay attention as you read this because you are going to start to see something so big that we could actually call it “the big picture”.
All cells exist within the context of a three-dimensional microenvironment in which they are exposed to mechanical and physical cues. These cues can be disrupted through perturbations to mechanotransduction, from the nanoscale-level to the tissue-level, which compromises tensional homeostasis to promote pathologies such as cardiovascular disease and cancer. The mechanisms of such perturbations suggest that a complex interplay exists between the extracellular microenvironment and cellular function.
Furthermore, sustained disruptions in tensional homeostasis can be caused by alterations in the extracellular matrix, allowing it to serve as a mechanically based memory-storage device that can perpetuate a disease or restore normal tissue behaviour. Thus, the physical basis for disease can be a product of either altered tensional homeostasis, owing to, for example, altered cellular-level or tissue-level forces and material properties, or the perturbed cellular response to mechanical stimuli.
Consequently, it is important to understand the functional link between the sensing of mechanical cues and the subsequent biochemical response, a process termed mechanotransduction, as this relationship is important for the maintenance of tensional homeostasis and for normal tissue structure and function.
Stop and grasp what these authors are saying (the lead author was Dr. Valerie Weaver of the Valerie M. Weaver Lab at UCSF’s Center for Bioengineering & Tissue Regeneration — the other two were a Professor of Chemical and Biomolecular Engineering, and a Postdoctoral Research Fellow in the field of analytical chemistry). This is exactly why I’ve shown you previously that increasing numbers of mega-intelligent people are touting aberrant mechanical homeostasis (much of it in the FASCIA SYSTEM) as the basis of all sickness and disease (HERE).
The authors went on to say that, “Remodelling of the ECM could function as a type of retention mechanism, whereby the physical microenvironment of the diseased state is preserved so that circulating tumour cells in tissues adjacent to the site of the primary tumour promote disease recurrence.”
In other words, if the body is allowed to “remodel” itself in an aberrant fashion, the result is sickness, disease, and CHRONIC PAIN. It’s why the way I treat patients (TISSUE REMODELING) is so crazy effective (HERE). In other words, the “remodeled” aberration must be “re-remodeled” back to normal. And what’s one of the end results of all of this inflammation and fouled up HOMEOSTASIS? Can anyone say CANCER?
CANCER, FIBROSIS AND THE ECM
Not too long ago I wrote an article on the relationship between FASCIA AND CANCER, but there are always new studies and new ways to look at old studies — new paradigms. Speaking of new paradigms, a study published in a 2014 edition of BMC Cancer (Epistemology of the Origin of Cancer: A New Paradigm) echoed what Dr. Seyfried said in the video embedded in the previous link — that chasing genetic mutations is about as effective as a dog chasing it’s tail. In other words, we are looking in the wrong place for the cure for cancer — RANDOM GENETIC MUTATIONS. Listen carefully to what these authors reveal (BTW, this paper cites 215 studies in its bibliography).
Fewer than 10% of all cancers are hereditary (only 15% of sporadic cancers are traced to somatic mutations). Carcinogenesis is widely thought to originate from somatic mutations and an inhibition of growth suppressors, followed by cell proliferation, tissue invasion, and risk of metastasis. We propose a new paradigm for the origin of the majority of cancers. Our paradigm postulates that cancer originates following a sequence of events that include….
(1) a pathogenic stimulus (biological or chemical) followed by…
(2) chronic inflammation, from which develops…
(3) fibrosis with associated changes in the cellular microenvironment. From these changes a…
(4) pre-cancerous niche develops, which triggers the deployment of…
(5) a chronic stress escape strategy, and when this fails to resolve….
(6) a transition of a normal cell to a cancer cell occurs.
Dr. Weaver, whom we discussed earlier, said almost the same thing in a study her team published in Trends in Cellular Biology (Forcing Form and Function: Biomechanical Regulation of Tumor Evolution). “Tumors are composed of a heterogeneous collection of cells surrounded by various soluble factors and an evolving extracellular matrix (ECM). In addition to the roles of genetic and biochemical events in tumor development, recent studies support the notion that biomechanical factors also critically direct tissue development, sculpt tissue organization and maintain tissue homeostasis.”
They also showed how these microscopic changes in tissue mechanics cause a change in tissue polarity — of critical importance, and why I have come to recommend some sort of routine(s) to supply yourself with electrons (HERE is a great example).
Dr. Weaver was back for the attack with another study, this one in a 2014 issue of EMBO Reports (The Extracellular Matrix Modulates the Hallmarks of Cancer). Listen to this extremely cherry-picked version of the study’s abstract.
“The extracellular matrix regulates tissue development and homeostasis, and its dysregulation contributes to neoplastic progression [cancer]. The extracellular matrix serves not only as the scaffold upon which tissues are organized but provides critical biochemical and biomechanical cues that direct cell growth, survival, migration and differentiation and modulate vascular development and immune function. Thus… cancer progresses within a dynamically evolving extracellular matrix that modulates virtually every behavioral facet of the tumor cells and cancer-associated stromal cells.
Hanahan and Weinberg defined the hallmarks of cancer to encompass key biological capabilities that are acquired and essential for the development, growth and dissemination of all human cancers. These capabilities include sustained proliferation, evasion of growth suppression, death resistance, replicative immortality, induced angiogenesis, initiation of invasion, dysregulation of cellular energetics, avoidance of immune destruction, and chronic inflammation.”
She goes on to talk about the extremely fibrotic nature of cancer, and the fact that it is heavily associated with “abnormal accumulation of collagen” within the ECM.
If you get cancer and decide to treat in standard medical fashion, at the very least you will get chemotherapy and radiation treatment. Although these can both kill tumor cells, both are also extremely carcinogenic. In other words, the treatment itself is a significant cause of cancer. Once we realize that under certain conditions, fibrosis can act as a sort of scaffold for cancer (see previous paragraph), this study from a 2015 issue of the Journal of Cancer Research and Clinical Oncology (Radiation-Induced Fibrosis: Mechanisms and Implications for Therapy — it was done at KU Med, MY BROTHER’S med school alma mater) will make more sense.
“Patients with cancer often receive external beam ionizing radiation therapy… Ionizing radiation induces damage not only in rapidly proliferating tumor cells but also in normal tissue in the radiation field. One important late effect that is a significant contributor to patient morbidity is radiation-induced fibrosis (RIF), which may occur in the skin and subcutaneous tissue, lungs, gastrointestinal and genitourinary tracts, as well as any other organs in the treatment field. Radiation injury triggers inflammation and ultimately stimulates transdifferentiation of fibroblasts into myofibroblasts. In addition to their excessive proliferation, these myofibroblasts
produce excess collagen and other extracellular matrix (ECM) components, which is compounded by a reduction in remodeling enzymes. Subsequent fibrosis reduces tissue compliance and—in a majority of cancer patients and particularly those with head and neck cancer—causes cosmetic and functional impairment that significantly impacts quality of life.”
As for chemotherapy-induced fibrosis / cancer, the amount of information I found is overwhelming. A study by ten European authors and published in Hepatology (Matrix Stiffness Modulates Proliferation, Chemotherapeutic Response and Dormancy in Hepatocellular Carcinoma Cells) concluded that, “Increasing matrix stiffness promotes proliferation and chemotherapeutic resistance.”
The word ‘proliferation’ simply means that the cancer is spreading / growing. The Canadian Cancer Society put it this way. “Some chemotherapy drugs can affect the lungs (pulmonary toxicity). It may be that the drugs cause inflammation in the lung cells that result in a lung infection. The drugs may also cause fibrous, scar-like tissue to form in the lungs (pulmonary fibrosis) and restrict lung function.”
This was echoed in the British Lung Foundation’s article, Drug-Induced Pulmonary Fibrosis in an almost verbatim fashion. In 2014, Frontiers in Pharmacology (Mechanisms of Cellular Fibrosis Associated with Cancer Regimen-Related Toxicities) had this to say on the subject.
Fibrosis is a common, persistent and potentially debilitating complication of chemotherapy and radiation regimens used for the treatment of cancer. The molecular mechanisms underlying fibrosis have been well studied and reveal overall processes that are largely ubiquitous. Data generated from animal models of cancer therapy-related tissue toxicities have revealed that the signaling pathways involved in fibrosis are the same as those involved in the normal injury response and include the transforming growth factor β superfamily and a range of pro-inflammatory cytokines.
The critical difference between normal wound healing and fibrosis development appears to be, that in fibrosis, these signaling pathways escape normal cellular regulation. As a result, an injury state is maintained and processes involved in normal healing are usurped. There are a few, if any, therapeutics that effectively prevent or treat fibrosis in patients. Consequently, cancer survivors may be chronically plagued with a variety of life-altering fibrosis-related symptoms.
In studying this issue, I discovered an interesting debate about whether or not to give these “ineffective” anti-fibrosis drugs to chemo patients in hopes that the chemo can break through the supposedly weakened fibrous barrier and into the tumor (it seems that many, if not most tumors, tend to have this fibrous barrier). For years I’ve heard that this fibrous barrier is there to halt (or at least slow down) the spread of cancer to other areas of the body.
A great example of this argument is found on pages 322-324 of Cancer Targeted Drug Delivery: An Elusive Dream. “We have previously argued that anti-fibrotic therapies at advanced stages could be a double-edged sword. In our opinion it is not certain whether fibrosis acts only as a barrier for chemotherapy, or also acts as a barrier against tumor spread.”
For the record, this 2013 book was not authored by “alternative” folk, but by three pharmacology / biomedical engineer, research types. Also for the record, it helps explain why biopsies can be deadly — they pierce the body’s walled-off tumor, potentially opening the encapsulation and releasing cancer cells into the general circulation.
SO, WHAT ARE YOU GONNA DO ABOUT FIBROSIS?
The question now becomes, what do I do about this mess? Before sitting down to CREATE YOUR WRITTEN PLAN OF ACTION, you must grasp is that successfully addressing inflammatory diseases including autoimmunity and cancer, no matter how it’s done, is difficult. That’s why prevention is a far better option than treatment after-the-fact. As for what you need to be doing, in either case it’s really not hard to see where you need to start by looking at the common threads found in these studies. The first action step you n
eed to take is to move (remember that both fibrosis and cancer are not simply biochemical, but biomechanical entities). And more importantly, you need to move in ways that address both strength (HERE) and your body’s proprioceptive abilities (HERE). Secondly, you have to deal with SYSTEMIC INFLAMMATION.
I’ve shown you in a bunch of posts (THIS ONE and THIS ONE sum it up pretty well) that inflammation always leads to fibrosis, and fibrosis not only leads to degenerative arthritic conditions, but as you saw today, results in an unholy hodge podge of nasty medical conditions and diseases — something that people way smarter than I am have been talking about for a very long time (HERE).
Fortunately, there are excellent ways of addressing some of these issues that I have put together for you. It’s not foolproof and it’s certainly not meant to diagnose, treat, or cure any diseases — according to the FDA, that is the sole realm of the practice of medicine. My protocol is simply meant to restore some harmony (homeostasis) to your body so that it can do what it was created and designed to do from the beginning — heal itself.
The doubly cool thing for you is that I give it to you as a free gift. No strings attached. Why? Because I feel so strongly that if you’ll study THIS POST, it holds the answers for the majority of you reading this. No; not all of you. The majority of you. And best of all, it won’t make you worse like so many medical treatments will (HERE). It’s almost the first of the year — take a look at it today and start taking your life and health back. What have you got to lose? Oh; don’t forget to reach out and touch us via FACEBOOK (like, share or follow) as it’s the easiest way to reach those you love and care about most!
