
CHRONIC NECK PAIN, DIAGNOSTIC ULTRASOUND, FASCIA & HYALURONIC ACID
|
|
Diagnostic Ultrasound as a technology is improving rapidly. There are now the 3D (still pics) and 4D (motion scans) that might eventually prove to be key in unlocking some of the mysteries that have plagued the medical community for so long regarding the role of FASCIAL ADHESIONS in CHRONIC PAIN SYNDROMES.
Enter Dr. Stecco.Famed Fascia researcher, DR. ANTONIO STECCO (an Italian MD) published a study not quite a year ago in the Journal of Surgical and Radiological Anatomy (Ultrasonography in Myofascial Neck Pain: Randomized Clinical Trial for Diagnosis and Follow-up) that came to some rather interesting conclusions. Because Fascia is so difficult to image and because we know that “Soft Tissues” are a universal component of Chronic Neck Pain, Dr. Stecco and his team said that, “A definitive diagnosis of chronic neck pain is sometimes not possible“. In other words, other than pain (which is subjective), our current imaging techniques frequently cannot objectively quantify what might be causing a person’s pain (HERE and HERE as well). The reality of this situation is that most people with problems that can’t be seen or touched are not taken seriously. They are all too often looked at as malingerers, drug seekers, or suffering from ‘Psychosomatic Delusions’ (it’s all in their head — i.e. even though it’s not PC to put it this way, they’re nuts).
For this study, Stecco had two groups of individuals — those with Chronic Neck Pain, and those without (“healthy”). They not only found that the “healthy” group had THINNER FASCIA than the “pain” group prior to treatment, they found that they could actually decrease the thickness of the the Fascia in “pain” group via treatment, which consisted either of Dr. Stecco’s Fascial Manipulation Technique or a combination of
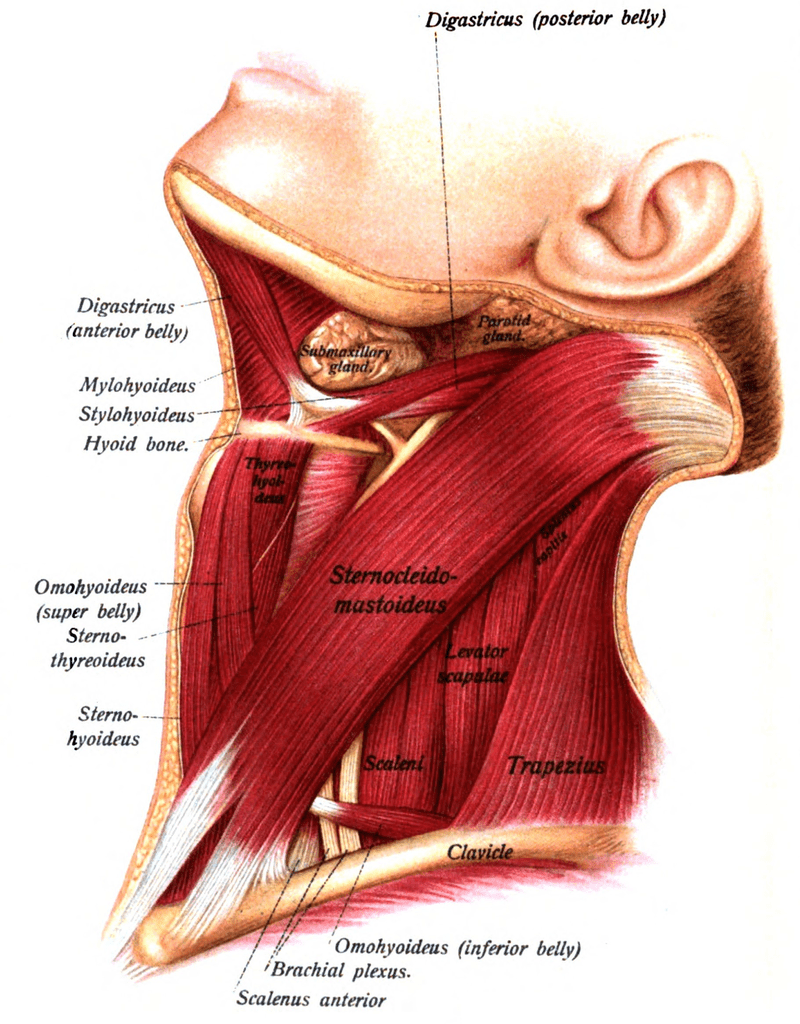
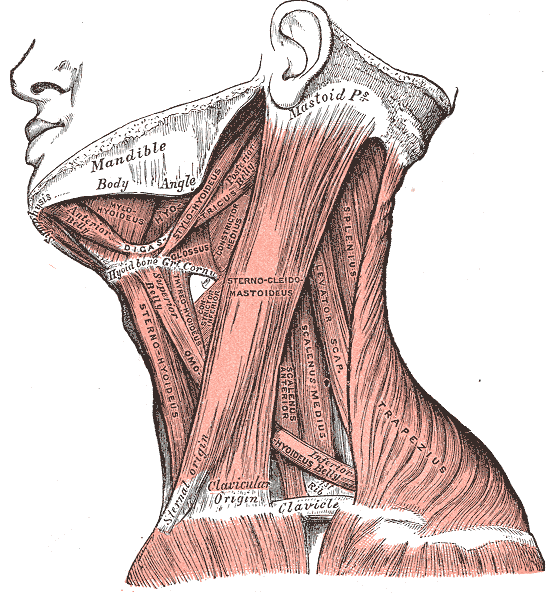
massage therapy, electrotherapy and LASER (for the record, the Fascial Manipulation proved more effective).By the way, the Fascia was tested from two different neck muscles — the Scalenes and SCM. The difference was not only seen immediately post-treatment, but upon a later follow up as well (A significant decrease in pain and thickness of the fasciae were found. Analysis of the thickness of the sub-layers showed a significant decrease in loose connective tissue, both at the end of treatment and during follow-up.). Experimentally, thinner Fascia has translated into better movement and diminished restriction, which as you might assume, translates to less pain as well.
The Ultrasound Videos I linked to earlier were by DR. HELENE LANGEVIN’S team, from a 2011 study called Reduced Thoracolumbar Fascia Shear Strain in Human Chronic Low Back Pain. In this study, the authors concluded that the Fascia of those with Chronic Low Back Pain not only moved significantly worse as seen in the short videos, but were actually 25% thicker. Much of this thickening and inability to slide (increased friction) is believed to do with something called HA or Hyaluronic Acid (aka
Hyaluronan or Hyaluronate) — a chief component of synovial fluid; the fluid that lubricates joints.As you might guess, HA has been targeted as both a drug and a nutritional supplement. When injected into joints, a meta-analysis (
Viscosupplementation for Osteoarthritis of the Knee: A Systematic Review) of several studies in the 2012 issue of the Annals of Internal Medicine revealed that, “viscosupplementation is associated with a small and clinically irrelevant benefit and an increased risk for serious adverse events” (for one, it’s a bio-marker for several types of CANCER). These are the “Rooster Comb” injections that people get in their worn out knees to try and buy them another year or two before they have to have them replaced (even though they often don’t work more than a few weeks).As far as using HA as a dietary supplement, it’s out there and being touted for everything from anti-aging to ARTHRITIS, to SKIN CONDITIONS, to BODYBUILDING, and just about any CHRONIC PAIN SYNDROME you could name. How effective are HA supplements? That depends on who you ask. Glucosamine Sulfate supplements have been around for a very long time and many people find these to be extremely effective (some contain HA). I am currently researching this topic for myself and will let readers know what I find. One thing I do know is that the current love affair with homemade “Bone Broth” soups cannot be anything but good for people’s joints and tissues (not to mention GUT). Listen to what Stecco and his team have to say about HA in the previously discussed study.
“…….in all overuse syndromes, an increase in the quantity of HA probably occurs in and on the surface of fascia. This may explain our findings. It is well documented that increased HA correlates not only with improved lubricating function, but also with increasing viscosity. Above all, it is organized on a surface. At high concentrations, HA behaves like a non- Newtonian fluid and becomes more viscous. At its most basic…the lubricant (HA) becomes less fluid, the loose connective tissues ‘thicken’…sliding functions reduce, and pain and restriction emerge. Treatment methods – manual or laser etc – that produce friction or heat, help to modify the viscous materials, and function improves….. Earlier studies by Langevin and colleagues [the one I linked to] have shown very similar changes in chronic low back pain patients… reduced sliding function, thicker loose connective tissue etc.“
Because Fascia is not a large area of study and because there are (at least not currently) no drugs for it, there has been relatively little interest in it. This, however, is beginning to change. For people who have not yet slipped into TYPE III PAIN, solving problems in the Fascia can prove to be life changing (HERE). And as is the case in virtually all health problems, DRYING UP THE UNDERLYING SOURCE(S) OF INFLAMMATION is key.
|
|
|
