
“Cervical pain is one of the most common symptoms in today’s society. Indeed, in our personal clinical experience, well over 90% of patients with headache have a cervical component easily observed with physical examination and which reveals abnormal cervical posture. Normal cervical posture presents with a lordotic curve of approximately 43 degrees measured from C2 to C7.1
Without this normal lordosis, most often the balance of the weight of the head is tilted forward and thus creates increased wear and tear on the intervertebral discs and the vertebral bodies. This eventually leads to bony spurs and osteophytes. Such changes also lead to decreased mobility of the cervical spine and to cervical pain.” From Springfield, Missouri’s very own pain expert, Dr. Norman Shealy (MD / Ph.D) from an article he wrote for Practical Pain Management back in April of 2009 (Restoration of Normal Cervical Curves).
“The lordotic curve of cervical spine radiographs was measured by analyzing the Cobb angle in 138 consecutive patients in a rheumatology office practice. All patients met the ACR criteria for fibromyalgia and complained of moderate to severe neck pain. 88% of fibromyalgia patients in this study had a straight neck based on measuring the Cobb angle, and 90% had a straight neck (loss of the lordotic curve) by visualizing the lateral view of cervical spine radiographs.
The cause of the straight cervical spine in fibromyalgia is unknown. Speculation of the pathophysiology [cause of fibromyalgia] includes chronic muscle contraction and tightness of other soft tissues.” From a paper (The Straight Neck in Fibromyalgia) presented by Dr. Robert Katz at last year’s Annual Meeting of the American College of Rheumatology
“Degenerative changes of the cervical spine are commonly accompanied by a reduction or loss of the segmental or global lordosis, and are often considered to be a cause of neck pain. Nonetheless, such changes may also remain clinically silent.” The opening sentences of a study called The Association Between Cervical Spine Curvature and Neck Pain from the May 2007 issue of The European Spine Journal
“In a healthy spine, the cervical lordosis looks like a very wide C, with the C pointing toward the back of the neck. This can begin to straighten in a condition called cervical kyphosis, in which the curve straightens up or even bows in the other direction. Sometimes this is referred to as “reverse lordosis,” referencing the fact that the spine is still curved, but the curve is now running in the wrong direction.” From What is Cervical Lordosis? on the website WiseGeek.
The REVERSE CERVICAL CURVE (also know as FHP or Forward Head Posture — a blatantly abnormal cervical curve) is nearly ubiquitous in our society. This is largely due to the absurd amount of time we spend sitting — and especially sitting hunched over a keyboard staring at at computer screen. Notice Wolff’s Law in action. You can see bone spurs beginning to form, discs beginning to thin, and calcium deposits being laid down, all due to carrying the brunt of the mass of the head on the front part of the cervical vertebrate instead of the back.
Although there is an abundance of scientific research showing a strong link between loss of the proper lateral curvature of the neck and a variety of health issues, including pain, we know that some cases (as the quote from the top indicates) are “clinically silent“. In other words, not everyone who has degeneration of the cervical spine (neck) is going to have pain (HERE). And likewise, not everyone who has pain is going to have degeneration. It’s what makes imaging (X-ray, MRI, CT, etc) dicey as far as being able to pinpoint an exact reason for a person’s pain.
Unfortunately, many of you who have been living on the MEDICAL MERRY-GO-ROUND understand this all too well. While none of this could be considered “new” information, it is information that is almost universally ignored by the practicing medical community. It’s another one of those areas where the gap between the way that physicians are treating patients in their clinics, and the discoveries that researchers are making in their labs, could be likened to the GRAND CANYON. Enter Dr. Mark Payne.
Dr. Payne is a retired Alabama Chiropractor, who, back in 1988, started a company dedicated to the manufacturing of quality equipment to restore abnormal cervical curves (Matlin Manufacturing, Inc). Dr. Payne follows Don Harrison’s Chiropractic Bio-Physics (CBP) Technique, and in 2008 wrote a 60 page booklet called The Best Corrections of Your Career: An Introduction to Postural Chiropractic. Dr. Mark sets out the premise of the book by revealing to chiropractors that,
“Failing to deliver real and meaningful corrective care to our patients is a real tragedy in terms of their long term health…. The laws of physics dictate that abnormal posture will harm your patients in any number of very real ways. When you relieve the pain but fail to to correct the underlying structural deficits you are shortchanging your patients and the consequences are very real and predictable.”
He then gives the book’s “Five Principles”.
- NORMAL IS NECESSARY
- POOR POSTURE IS SUBLUXATION
- ADJUSTMENTS ALONE CAN’T FIX IT
- YOU MUST HAVE ACCURATE AND REPEATABLE METHODS OF ANALYSIS
- YOU MUST HAVE THE RIGHT TOOLS FOR THE JOB
-NORMAL CERVICAL CURVE; NORMAL IS NECESSARY
The whole reason your body requires a “normal” lordotic cervical curve is to allow for normal joint motion — joints can only move correctly when normal structure is present. In an age of relativism, this can be a bitter pill to swallow — particularly if you do not have any overt symptoms or pain. In other words, many would have you believe that your “normal” is different than my “normal”. Not true.
Back in a 1959 study done by Borden, Hechtman, and Gershon-Cohen — all M.D.’s (The Normal Cervical Lordosis), began to answer this question of what makes up a normal cervical curve. And although the measuring method was dramatically different than today’s methods, their picture of what constitutes “normal” was just about identical to what would pass for normal today.
Although there have been numerous studies on this topic since, a 2005 study in the medical journal JMPT summed it up nicely in a study called Determining the Relationship Between Cervical Lordosis and Neck Complaints. Listen to what the authors wrote after sorting patients into two main groups — those with neck problems and those without.
“We found a statistically significant association between cervical pain and lordosis less than 20 degrees and a “clinically normal” range for cervical lordosis of 31 degrees to 40 degrees. Patients with lordosis of 20 degrees or less were more likely to have cervicogenic symptoms [symptoms arising from the neck]. The odds that a patient with cervical pain had a lordosis of 0 degrees or less was 18 times greater than for a patient with a noncervical complaint.“
In the years since Payne completed his short book, there have been great numbers of studies on this topic, many of which I covered HERE. Although many in the medical profession say it doesn’t matter, the range I seen bantered around as “normal” is 30 to 40 degrees (I believe it was Dr. Shealy who said that normal lordosis of the cervical spine was 43 degrees). If you wish to see what that this normal curvature looks like, just take another glance at the picture at the top of the page. You will begin to understand more about normal once you begin to learn more about abnormal.
-NORMAL CERVICAL CURVE; POOR POSTURE IS SUBLUXATION
SUBLUXATION is defined simply as bones (usually vertebrate) that lose their normal alignment or motion in relationship to each other. Study after study after study is verifying the devastating effects of poor posture / postural deformities on human health. I Googled “effects of poor posture research studies” and found studies linking postural abnormalities to diseases you would not suspect such as Type II Diabetes and High BP.
Some of the others specifically mentioned in the peer-reviewed research included things as diverse as fear, sadness, emotional instability, mental acuity, mood, energy levels, back pain, coordination, constipation, and even certain types of cancer. There is even research linking poor posture to shorter life span. What I really want you to notice here is how few of these problems that were mentioned have anything whatsoever to do with pain. Suffice it to say that FHP (Forward Head Posture) along with trunk flexion (THE POSTURE OF AGE) have tons of peer-review showing how detrimental they are to human health.
-NORMAL CERVICAL CURVE; ADJUSTMENTS ALONE CAN’T FIX IT
Chiropractors cringe at old standbys such as “How many chiropractors does it take to change a light bulb? Just one, but it will take him one year and 150 visits to do it.” We deserve to cringe. For decades, the profession has been telling patients that all they need to solve their problem is more adjustments (HERE). Don’t get me wrong; adjustments are extremely powerful (HERE).
The problem is, simply adjusting patients over and over and over again without any sort of tangible goal in mind other than short-term pain relief is playing the same game that the medical doctors play, only without the nutty side effects of DANGEROUS & DEADLY DRUGS OR PROCEDURES. Listen carefully as Dr. Payne rares back and punches the chiropractic profession squarely in the mouth.
“The ugly truth about chiropractic adjusting is that there is almost no evidence at all to suggest that adjustments alone do very much to actually correct spinal structure.” For those of you who didn’t get this the first time, a few sentences later he repeats himself. “There’s absolutely nothing in the scientific literature to indicate that you can actually change spines effectively with adjustments alone.”
He then says why. “The answer is painfully obvious to professionals in other fields like university biophyisics and biomedical engineering who are engaged in studying the more technical aspect of the human machine.” In other words, chiropractors have failed to comprehend the importance of certain physical properties that all living tissues possess, “elasticity, viscosity, plasticity, and strength“. We (my profession) have collectively failed to grasp just how big a role that physics (BIOMECHANICS) plays in solving the problem of abnormal spinal curves.
When I graduated from Logan Chiropractic College back in 1991, the big emphasis was on restoring joint motion. Not that this is a bad thing but me learning that restoration of joint motion (primary) takes care of joint misalignment (secondary) was about 180 degrees opposite of the truth.
Don’t get me wrong; restoration of motion (BOTH SECTIONAL AND SEGMENTAL) is critically important and can bring about rapid pain relief (HERE, HERE, and HERE are great examples of this). One of the chief things I like about our unique brand of Tissue Remodeling is the fact that it rapidly changes the VERY PHYSICS OF SCAR TISSUE so that long-term structural correction is easier to make — much easier to make. However, it’s important to understand that pain relief is not where the process ends for people wanting to live a long, fruitful, productive, and pain-free life.
-NORMAL CERVICAL CURVE; YOU MUST HAVE ACCURATE AND REPEATABLE METHODS OF ANALYSIS
This isn’t exactly rocket science. There are essentially two different aspects to this bullet point. Visual Postural Analysis and / or X-rays. The more accurate of the two will almost always be X-ray. I also love to use RANGES OF MOTION. This is simple to check, takes all of about 10 seconds to do, and in most cases, will tell me exactly where I need to focus my attention — particularly with Tissue Remodeling.
-NORMAL CERVICAL CURVE; YOU MUST HAVE THE RIGHT TOOLS FOR THE JOB
Thus far we have learned that there is a “normal” amount of cervical curve that you should have in order to up your odds of avoiding a myriad of health-related problems as well as chronic pain. Furthermore, we know that simply getting adjusted over and over and over again is never the solution.
In order to restore an abnormal curve, you are going to have to engage in activities / forms of treatment that actually change the physical properties of the tissue mentioned a few paragraphs earlier — things that actually cause TISSUE DEFORMATION. This takes time. Not time as in month after month of adjustment after adjustment — adjustments that each last no more than a fraction of a second. But time as in changing tissues by stretching them into a normal position. Dr Payne puts it like this. “What we really need are ways to apply sustained corrective forces for a sufficient time to change the soft tissues.”
This can be largely accomplished at home using the DAKOTA HOME TRACTION or COMPRESSION-COUNTER STRESSING TRACTION aka “The Stynchula Method” (Payne wants you to slowly work your way up to as much as a half hour a day). I think he’s spot on.
It was Dr. Rene Calliet’s 1987 book Rejuvenation Strategy that stated, “Most attempts to correct posture are directed toward the spine, shoulders and pelvis. All are important, but, head position takes precedence over all others. The body follows the head. Therefore, the entire body is best aligned by first restoring proper functional alignment to the head“. Dr. Calliet was the Director of Physical Medicine and Rehabilitation at USC’s School of Medicine at the time he wrote this.
NORMAL CERVICAL CURVE -VS- ABNORMAL CERVICAL CURVE: CONSEQUENCES OF SUBLUXATION / ABNORMAL CERVICAL CURVE
This, folks, is where the rubber meets the road. As the study at the top of the page said, some cases of subluxation / abnormal cervical curve are “clinically silent“. In other words, because they might not be producing any overt symptoms, most people (physicians included) would not consider them as important or harmful. However, there are four symptoms that come up time and time again not only in the scientific literature, but in the clinical setting as well, that are associated with abnormal curvature of the cervical spine. These four are….
- ABNORMAL RANGE OF MOTION
- PAIN
- NEUROLOGICAL ISSUES
- DEGENERATION
-ABNORMAL CERVICAL CURVE; ABNORMAL RANGE OF MOTION
I have written about what constitutes normal ranges of motion in the cervical spine (HERE), and the consequences of not having this curve. The biggest thing I want you to understand in this bullet point is that the proper lordotic curve allows “coupled motion” in the vertebra of the neck. Clear back in 1993, the brilliant spinal biomechanist Dr. Manohar Panjabi published a study in The Journal of Orthopedic Research called Posture Affects Motion Coupling Patterns of the Upper Cervical Spine. Very technical information, if you care to read it.
More recently in 2004, Physical therapist Gary Gray wrote that, “Functionally understanding that movement in any one plane of the vertebral column is accompanied by movement in the other two planes. With the three dimensional capacity of the cervical spine, the three dimensional spinal coupling concept is significant. Even when we load a bobble-headed doll in one plane of motion, it reveals that plane of motion plus the other two as it “bobbles its head”.”
How complex are these coupled motions in the cervical spine? A Chinese study last year (Three-Dimensional Analysis of Cervical Spine Segmental Motion in Rotation) was published in Archives of Medical Science stating that, “The movements of the cervical spine during head rotation are too complicated to measure using conventional radiography or computed tomography (CT) techniques“.
-ABNORMAL CERVICAL CURVE; PAIN
Pain sucks — especially if it is chronic (long term, relentless) pain. And unfortunately, the medical community’s approach to dealing with CHRONIC PAIN is not known for having a fantastic success rate. I mean, let’s be brutally honest with ourselves for a moment. Are PRESCRIPTION PAIN MEDS, NSAIDS, MUSCLE RELAXERS, CORTICOSTEROIDS, and ANTIDEPRESSANTS going to help a patient over the long haul who is struggling on a day-to-day basis with neck pain? How could they when they are not even attempting to address underlying cause(s)?
Bear in mind that while it’s usually pain that motivates people to come see me, it’s often the easiest of the four bullet points to deal with. By the way, I am not minimizing your pain. It’s just that there may be more to solving your problem than simply relieving your pain. After all, if pain relievers truly worked, you wouldn’t be reading this post at 3 am with tears in your eyes.
-ABNORMAL CERVICAL CURVE; NEUROLOGICAL ISSUES
This one covers a lot of ground. Technically, pain could have also been lumped into this class, as could things like RADICULOPATHY, most HEADACHES, and a large percentage of MIGRAINES. The bottom line is that a “Head Forward Posture” puts large amounts of excess mechanical stress on the cervical spine — particularly the front (anterior) portion of the cervical spine.
Clear back in 1974, Dr. Adalbert I. Kapandji, an orthopedic surgeon, wrote in his famous textbook, The Physiology of Joints, that, “for every inch of Forward Head Posture, it can increase the weight of the head on the spine by an additional 10 pounds.” A few years later in 1978, Nobel Prize winner and Swedish neurosugeon, Dr. Alf Brieg, published a study in JAMA (the Journal of the American Medical Association) called Adverse Mechanical Tension in the Central Nervous System: An Analysis of Cause and Effect; Relief by Functional Neurosurgery.
The paper’s abstract (he also published a book by the same name) started out by saying that, “Hidden behind this forbidding title is a text that is radical, revolutionary, and incredible. It gets at the roots of things, should overturn cherished concepts, and parts of it are difficult to believe. Using cadaver, animal, and clinical material, Breig shows how tension in the brain, brain stem, spinal cord, and nerve roots can give rise to local and distant signs and symptoms. There are ample illustrations of the mechanical analyses and principles that are used to support his therapeutic suggestions and practice.”
The study went on to say that some of these signs and symptoms are specifically caused by “abnormal tensile forces” in the cervical spine. Breig’s list includes things as diverse as, “facial neuralgias, spasticity [TRIGGER POINTS], bladder dysfunction, as well as cervical and lumbar spondylosis, disk hernias, trauma to the spinal cord, confusional states, and multiple sclerosis.” This is yet another example of “Subluxation” and / or postural deformities leading to a wide variety of symptoms that are seemingly unrelated to the spine. If you want to see a radical example of Subluxation’s effect on neurology, take just a second and READ THIS.
-ABNORMAL CERVICAL CURVE; DEGENERATION
Degeneration is the visible finale of abnormal biomechanical stresses over time that can be seen on imaging tests such as X-ray or MRI — even though IT MIGHT NOT MEAN WHAT YOU THINK IT DOES. If you were to go back and look at the picture of the normal cervical curve at the top of the page, the first thing you would see is the “forward curve”. This forward curve is critical because it is not only the very thing that allows coupled motions of the neck to occur, but it acts as a shock absorber as well. Springs are curves that bounce back, and the normal curve in the neck acts as a spring.
Furthermore, the neck is created and designed so that the mass of the head is carried on the Facet Joints that glide on each other and are found at the back (posterior) portion of the spinal column. As the neck loses its normal curve (or especially if the curve actually reverses), the head’s mass will be carried on the fronts of the vertebral column instead of the rear.
To help you understand this, take a look at the pictures of the Reverse Cervical Curves below). These abnormal curvatures will virtually always lead to degenerative changes such as bone spurs, calcium deposits, and thinning discs. Despite what doctors want you to believe, this is not so much a “DISEASE,” but the result of something called “Wolff’s Law”.
Wolff’s Law says that bone grows / remodels in response to mechanical stresses put on it, whether said stresses are normal or abnormal. This is why doctors put people with broken legs in “walking casts” as soon as possible in order to facilitate bone growth and healing. It is also why some areas of a skeletal system are much thicker or knobbier than others. Where muscles attach to bone and pull at them constantly — especially powerful muscles — the attachment points will be enlarged / thickened. Dr. Payne does not mince any words when talking about Wolff’s Law.
“Want to know why your patients absolutely, positively, must regain structural balance in order to have good health? It’s because gravity is a complete bitch. Like Schwarzenegger’s Terminator character, it can’t be reasoned with, it has no pity, and it won’t ever, ever stop. If you don’t do something to restore the normal structure of your patient, the end game has already been decided.“
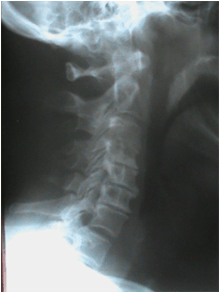
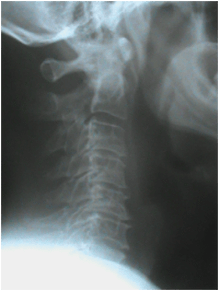
(ABNORMAL CERVICAL CURVE) X-RAYS OF THE REVERSE CERVICAL CURVE
 |  |  |  |  |
-ABNORMAL CERVICAL CURVE; CAR WRECKS AND LOSS OF THE
One of the most common ways to really foul up a cervical curve is to be involved in a MVA (MOTOR VEHICLE ACCIDENT). MVA’s — especially rear-enders — cause serious injuries to the body’s soft tissues (MUSCLES, LIGAMENTS, TENDONS, and most particularly, FASCIA —- especially in the SCM), and can defy most treatment approaches (HERE).
Determining whether someone has had some sort of “WHIPLASH” injury (whether caused by a car crash or not) is fairly simple. When you see disc thinning in the lower C-spine — most particularly at the disc between C5 and C6 — you can bet your bottom dollar that there was a “hyperextension / hyperflexion” injury (whiplash) involved.
The films below are both of middle aged women who each presented with CHRONIC NECK PAIN, and a history of being rear-ended years previously. Notice the beak-like bone spurs and thinning taking place at the C5-C6 disc space. Again, inordinate amounts of decay at C5-C6 indicates that a whiplash-like injury took place there at some point in time — quite possibly decades previously.
 |  |
DEGENERATION OF THE CERVICAL SPINE RELATED TO ABNORMAL CERVICAL CURVES
It’s a common excuse when you go to the doctor’s office. Your physician, after ordering a slew of tests to determine why you are having neck pain, sits you down, looks mournfully into your eyes and slowly tells you, “Mrs. Smith, we figured out what your problem is. You just aren’t as young as you used to be“. The implication, of course, is that Spinal Degeneration is primarily a function of age. This is BS of the highest order.
Sure; if you live long enough, you are going to end up with some degenerative changes in your spine. That’s called life (NOT TO MENTION INFLAMMATION). However, trying to pin all of a person’s pain on degeneration is not only a cop out, but usually the easiest excuse to get you out of their office and into the pharmacy so that you can pick up the prescriptions (PLURAL) that are waiting for you.
One more quick note here. Degeneration is not the end of the world. It would shock many people (therapists and chiros included) just how much range of motion can actually be restored by breaking up Scar Tissue and Fibrosis — sometimes even in people you would swear already had “normal” ranges (HERE). All of this is why you cannot skip PHASE I and go straight to PHASE II — something numerous practitioners do. Neither can you live in Phase I like many chiros tend to do. It’s all about doing the right things in the right order (HERE).
These are some pics of x-rays (all are lateral pictures of the neck, and all are facing to your right). Notice the bone spurs, calcium deposits, and thinning discs (some areas are literally fused together because the discs are gone). Also notice the funky curves. These were a few that were randomly pulled from my files when I was getting rid of x-rays that were over a decade old.
 |  |  |
  |   |   |
If you are interested in real results without tons of drugs, take a look at at few of our VIDEO TESTIMONIALS. An approach that deals with INFLAMMATION & SCAR TISSUE, and helps restore normal movement and alignment of the spine is effective for helping many people not only get out of pain today, but normalize their biomechanics so that they stay out of pain, while allowing their body to function optimally. For those of you struggling with a variety of chronic health issues, take a moment to look at THIS POST.
