
OpenStax College “If a scar is thick and deep, it can limit movement and cause pain.”From physical therapist Cynthia Neville’s June 2013 article for the Rehabilitation Institute of Chicago (Scar Management: Massage after Abdominal Surgery). If you read the quote from Neville at the top of the page, you might assume that this is ANOTHER POST on post-surgical Scar Tissue. It’s not. In some ways the post-surgical abdomen is easier to deal with simply because the scar is, as Neville says, “thick and deep“. In other words, it’s visible. But what about those problems where there was no surgery or injury that quickly comes to mind (C-sections, hernia repair surgeries, organ transplants or removals, intestinal surgeries, difficult pregnancies or deliveries, blows, beatings, severe twisting injuries, etc, etc)? And what then happens when no one in the medical community can really tell you what’s wrong with you? Or worse yet, thinks you’re faking it to get drugs or disability? That is the topic of today’s post.
It’s not uncommon for me to see people with STRETCHED, PULLED, OR TORN MUSCLES. The thing you have to remember is that rarely is a muscle really “torn”. What I mean is that it is not common to tear the muscle belly — the meat of the muscle —- even though that sort of language is used routinely. Most of these problems involve tears of the FASCIA (the thin, clearish-yellow, cellophane-like membrane that covers the muscle), and not the muscle itself.
For whatever reason(s) (SPORTS, MVA, falls, the things listed above) a person ends up with an abdominal problem. The sort of problem I am wanting you to get a picture of not only causes pain, but most frequently it causes at least some degree of lost motion and / or strength as well. We once had a phenomenal high school athlete brought in to us in a wheel chair with an abdominal “tear” that happened while playing Ultimate Frisbee (no rough stuff; he just came down wrong). Regardless of how it happened, whether it’s a new injury or old, or how debilitating it might seem at the moment; knowing more about this common injury might help you get your life back on track or at the very least, save you some future grief. Allow me reveal to you some facts that make this and similar injuries not only potentially debilitating, but nearly impossible for the average doctor to figure out.
- THE AVERAGE DOCTOR HAS NO IDEA HOW TO DIAGNOSE THESE SORTS OF PROBLEMS: As you might imagine, the first step in providing effective treatment is to have some sort of idea what the problem is. This means providing a proper diagnosis. Rather than me telling you, HERE is a post that contains a study letting you know just how poor a job general doctors do diagnosing musculoskeletal problems in the first place.
- THE AVERAGE DOCTOR HAS NO IDEA HOW TO TREAT THESE SORTS OF PROBLEMS: I wrote about this YESTERDAY. As you might also imagine, the usual drugs (CORTICOSTEROIDS, PAIN PILLS, and NSAIDS) are not going to do it. Fail to deal with the SCAR TISSUE in the Fascia and sooner or later you will be suffering. Unfortunately, tests and drugs are what doctors do. Great for some things. Not so great for problems like this.
- MOST SCARRED ABDOMINAL TISSUE DOES NOT SHOW UP ON MRI: Mind you, I am not talking here about the sort of “internal” adhesions that are the result of female issues such as ENDOMETRIOSIS. I am talking about adhesions in the tissues — most specifically Fascia (although sometimes TENDONS are involved — think HIP FLEXORS here). I have shown you over and over on this site that Fascia does not image will with MRI (HERE are several posts attesting to this).
- FASCIA IS THE MOST PAIN-SENSITIVE TISSUE IN THE BODY: Not only is Fascia arguably the single most pain-sensitive tissue in your entire body, but according to Dr. Chan Gunn, a neurologist from the University of Washington, Scar Tissue has the potential to be “superconductive” (HERE is why). This means that Scar Tissue can actually be up to 1,000 times more pain-sensitive than normal tissue.
- SCAR TISSUE IS UP TO 1,000 TIMES MORE PAIN-SENSITIVE THAN NORMAL TISSUE: Whoops. We covered this in the previous bullet point. However, stop and ponder this fact for another moment or two. It’s easy to begin to see why the medical community is usually missing the boat in this department. Case in point; how many doctors have shared this information with you?
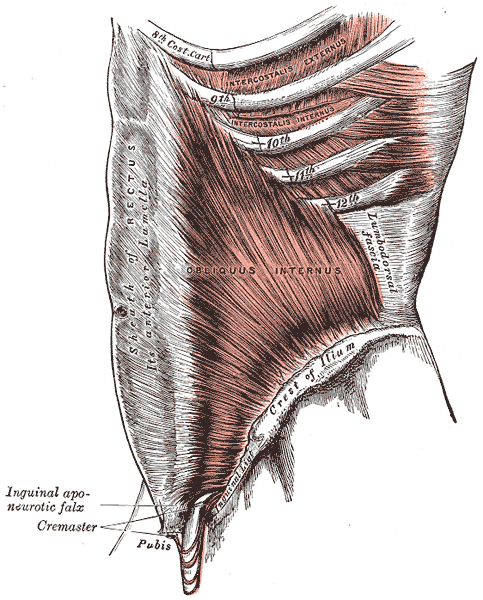
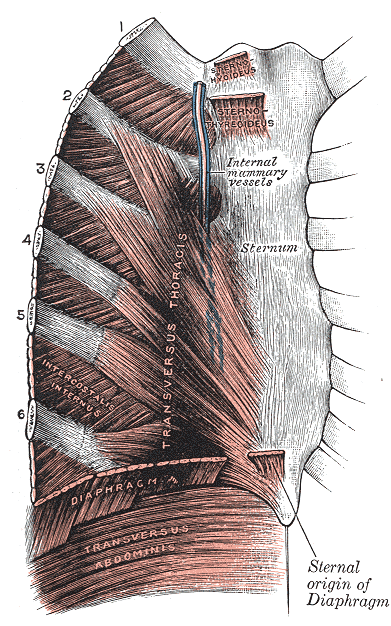
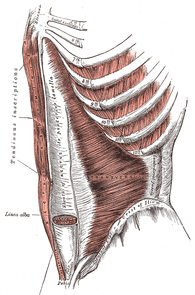
- THE NATURE OF THE ABDOMINAL MUSCLES THEMSELVES: The thing about the abdominal muscles is that they are made up of layers — lots of layers — one on top of the other, that all run in different directions. Look carefully at all of the pictures on this page. The very reason I put these pictures up is to show you that the abdominal muscles run up and down, side to side, and criss-cross (oblique) in both directions. And that’s just for starters.
 |  |  |
When you add all of these factors together, you can start to see why no one has been able to explain to you what’s going on. You can also see why it’s the “PERFECT STORM” of Chronic Pain. Don’t get me wrong; CHIROPRACTIC ADJUSTMENTS can be MIRACULOUS for a wide number of health-related problems. But if your abdominal problem has its roots in Scarred Fascia, I don’t care if you get adjusted every day until Doomsday, you won’t get the adjustment to hold more than a few days — sometimes only a few hours. I know, because this is exactly what my average long-distance patient with this particular problem has been through.
By the way, if you pay attention to the pictures, you can’t help but notice the intimate relationship between the ribs, the muscles on and around the ribs (intercostals, serratus, transversus thoracis, etc, etc) and the abdominal muscles. This is why I so frequently see these problems (RIB TISSUE PAIN and ABDOMINAL PAIN) living together in one big unhappy family (often times with their red-headed stepchild — HIP FLEXOR PROBLEMS). If you think that this might be your problem, send me a PATIENT HISTORY. If I think your problem is something I could help you solve, I’ll tell you. If not, I will tell you that as well (HERE). The first step is determining whether your problem is related to scar tissue in the abdominal wall or the abdominal cavity (HERE).
