
UPPER CROSSED SYNDROME
WHAT IS IT, WHAT CAUSES IT, WHAT DOES IT LOOK
LIKE, AND HOW TO EFFECTIVELY ADDRESS IT
 |  |  |
YESTERDAY I talked about Dr. Janda’s Lower Crossed Syndrome. Today we tackle the upper body’s analogous muscle imbalance pattern; Upper Crossed Syndrome. Like its counterpart, this biomechanically aberrant pattern has a great deal to do with FORWARD HEAD POSTURE — truthfully even more so. Without any further adieu, let’s start answering the questions posed by the title one at a time.
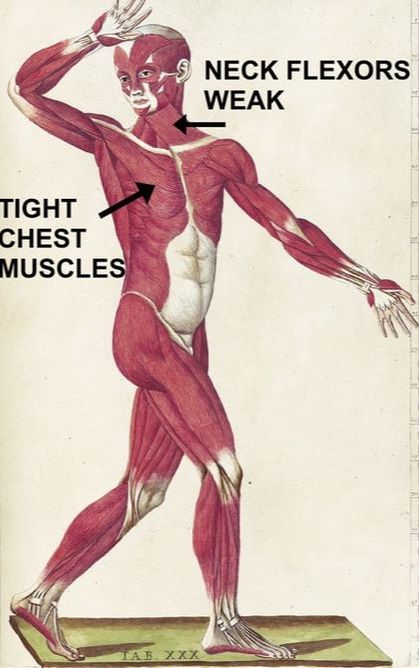
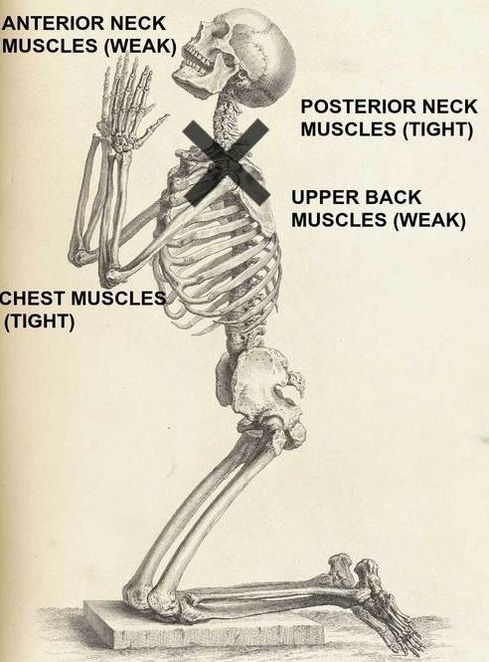
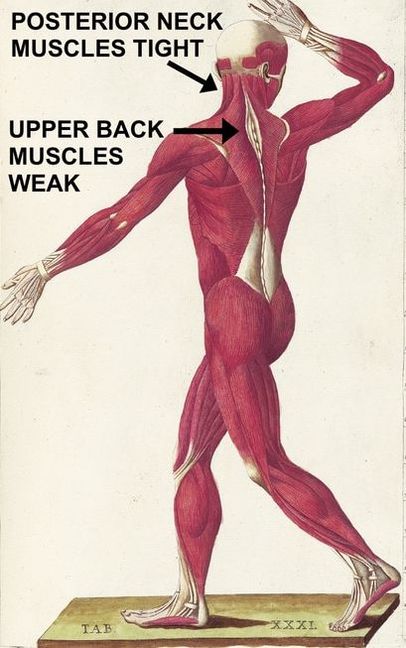
As seen by the pictures above, Upper Crossed Syndrome is where the chest muscles (pectorals) and rear neck muscles (upper traps, LEVATOR SCAPULAE, suboccipitals, and SCM, which in this context is considered a rear or at least a lateral neck muscle) are overly tight, while the upper back muscles (rhomboids, lower trapezius) and front neck muscles (PLATYSMA, SCALENES) are weak (or at least inhibited in their firing). According to Janda’s book Assessment and Treatment of Muscle Imbalance: The Janda Approach (as paraphrased by the group officially carrying on his work — The Janda Group at Muscle Imbalances dot com), Upper Crossed Syndrome leads to…..
“Dysfunction, particularly at the atlanto-occipital joint, C4-C5 segment, cervicothoracic joint, glenohumeral joint, and T4-T5 segment. Postural changes decrease glenohumeral stability as the glenoid fossa becomes more vertical due to serratus anterior weakness leading to abduction, rotation, and winging of the scapulae. This loss of stability requires the levator scapula and upper trapezius to increase activation to maintain glenohumeral centration (Janda 1988).”
Follow along as I show you why this is bad stuff, as well as how to start dealing with it on your own.
WHAT DOES UPPER CROSSED SYNDROME LOOK LIKE?
Like Upper Crossed Syndrome, the causes are many and varied, with many being similar. Much of this centers around the fact that POOR POSTURE is contagious. No; I don’t mean that you’ll spread it to your buddy like some kind of crazy disease. I mean that once you start having certain characteristics of poor posture in one area, it progresses to others. Things can slide downhill quickly as as thanks to compensation, the whole mess progresses (see link on FHP at the top of the page). Loss of normal spinal alignment causes loss of normal joint motion or movement patterns, which in turn leads to PHYSICAL DEGENERATION in the form of loss of joint space, calcium deposits in soft tissues, and bone spurs (osteophytes). There are other signs of Upper Crossed Syndrome.
- HUMPBACK: This, folks, is a no-brainer. If you have overly tight chest muscles pulling you forward and weak upper back muscles failing to resist their pull, you will be pulled forward. In other words, you’ll eventually end up battling FHP’s evil twin, “Hunchback” (I often times refer to this as “THE POSTURE OF AGE“). Sometimes these folks will actually have a normal-appearing (or even hyperlordotic neck) from holding their head up as the whole mess slides anteriorly (forward). After looking at thousands upon thousands of X-rays of the neck in profile (lateral cervical spine), over the course of twenty five years, all I can say is that cervical lordosis is rare. What’s common is that humpback and FHP are seen together, pulling people further and further forward, self-perpetuating the problem.
- VARIOUS KINDS OF SCAPULAR ABNORMALITIES: When you see winged scapulas or abnormal scapular positions of almost any kind, start to suspect Upper Crossed Syndrome.
- CHRONIC PAIN: Remember what I showed you several months ago (HERE) — that postural abnormalities over time are one of the many ways to create SCAR TISSUE / FASCIAL ADHESIONS / FIBROSIS / DENSIFCATION, or whatever else you choose to call it? Upper Crossed Syndrome also happens to be one of the prime factors in developing TRIGGER POINTS in the area of the upper back, pec minor, SCM, and levator — none are worse than the levator (see earlier link on the levator). Add Scar Tissue with Trigger Points and you have the “Myofascial Syndrome”. Thus, it is common to see people with Upper Crossed Syndrome dealing with HEADACHES, CHRONIC NECK PAIN, and various forms of RADICULOPATHY, including THORACIC OUTLET SYNDROME.
WHAT CAUSES UPPER CROSSED SYNDROME?
Honestly, this is largely the same group of actors we saw with Lower Crossed Syndrome. However, there are specifics here that need to be addressed.
- SITTING COMBINED WITH POOR POSTURE: Sitting itself is bad enough, but combine it with a slumped posture, and you are setting the table for future problems. In our age of computers, sedentary lifestyles, texting, etc, etc, this problem continues to grow.
- ABERRANT TRAINING PATTERNS AND REPETITIVE SPORTS: Unfortunately, I find that when it comes to physical training and activity, way too many people are doing things wrong. Often times darn drastically wrong. Allow me to give you a prime example. I never used to see serious shoulder problems in high school volleyballers. Now they’re common. Young teens (and even adolescents) serving and spiking who-knows-how-many-times, at least five, often six, and sometimes seven times a week. With the advent of longer seasons, summertime “open gym” sessions, and JO’s (Junior Olympics), these girls are going through what amounts to a pitching motion, hundreds upon hundreds of times a week. This is interesting in light of the fact that big league pitchers are on a five-day rotation, usually with a pitch-count limit of 100 or so, and after pitching, have the arm encased in ice and do all sorts of therapy until they pitch again.
- LARGE BUSTS: Large breasts have a tendency to pull women into a slumped or rounded-shoulder posture. My experience is that there comes a point where reduction may be necessary to achieve any sort of lasting relief. I can say that of my patients who have gone through reductions, I have yet to see one who regrets it.
EFFECTIVELY DEALING WITH UPPER CROSSED SYNDROME
Although lifting weights can be an integral part of solving Upper Crossed Syndrome, frequently it’s weightlifting that causes this problem (or at least heavily promotes it) in the first place. For instance, people love to work the muscles they can readily see in a mirror — chest, biceps, abs (almost always in the form of SITUPS), front shoulders, and quads, while ignoring (or at least minimizing) muscles they can’t see (upper back, lower back, glutes, and hamstrings).
What this tends to do — especially in the upper body — is cause a head-forward, shoulders-rounded, bent-forward, slumped sort of posture. This is why when it comes to dealing with Upper Crossed Syndrome, I’m a fan of focusing on posterior chain muscles, while limiting presses (benches / military) and doing a lot of EXTENSION TYPE WORK; as much on a ball as possible. Just remember, however, that exercises are not necessarily the best starting point. When it comes to solving this problem…….
- STUDY AND CREATE A WRITTEN PLAN — AN EXIT STRATEGY IF YOU WILL: There are so many articles and YouTube videos on the subject that while you may not be an “expert” with just a few hours of study, you’ll start seeing the bigger picture. EXIT STRATEGIES work, and like they say — failure to plan is planning to fail.
- DEAL WITH UNDERLYING SCAR TISSUE AND SUBLUXATION: Contrary to what most practitioners (PT or DC) say, this does not mean starting with lots of exercises (HERE) or adjustments (HERE) respectively. What it does mean is that you may need to deal with the effects of Scar Tissue (see earlier links) if it is present. Why is this important? Scar Tissue has a TETHERING effect that limits normal ranges of motion. Loss of motion, or abnormal motion patterns sooner or later lead to pain. But unfortunately, pain is not where this little shindig ends. The end product of Upper Crossed Syndrome is always the degeneration I spoke of earlier.
- TREAT THE PROBLEM AS THOUGH IT WERE SYSTEMIC: Look; I’m not going to tell you that changing your diet, giving up the SMOKES, taking care of your GUT, and starting an exercise program are automatically going to “cure” your Upper Crossed Syndrome. However, if you can effectively and naturally deal with INFLAMMATION — particularly SYSTEMIC INFLAMMATION — you are better off. This is a cold, hard fact that is always true 100% of the time.
- STRETCHES AND EXERCISES: I’m not going to give you tons and tons of specifics here as there are many other sites that have done a far better job than I. I will, however, give you some tidbits to chew on. For starters, before starting, make sure you understand LOWER CROSSED SYNDROME and it’s relationship to CORE STRENGTH. I also suggest you learn to do what I call the Chicken Head Move. Huh?
- CHICKEN HEAD MOVE (CHIN TUCK) WITH SCAPULAR RETRACTION: Growing up on a Kansas farm, I’ve seen plenty of chickens bobbing their heads back and forth as they move. When you do a Chin Tuck, tip your chin slightly downward (I did say slightly). Now take your chin in your hand and move it forwards and backwards CHICKEN HEAD STYLE. Ultimately, what you want to do here is be able to control the muscles that allow you to tuck your chin back as far as you can get it. Then retract your scapulas — pull your shoulder blades back towards each other. Practice this and make it your go-to posture for dealing with Upper Crossed.
- OTHERS: Frankly, there are so many cool exercises and stretches for Upper Crossed Syndrome that I could write a book. Again, search the web. In the meantime, I included a little slide show of some of the exercises and stretches that might be of benefit (yes, I realize that some of these will need to be modified for the average person). And because there is so much overlap, make sure to at least look at the exercises and stretches used for people with Lower Crossed Syndrome.
