
LOWER CROSSED SYNDROME: WHAT IS IT, WHY IS IT A PROBLEM, AND HOW SHOULD YOU BE ADDRESSING IT?
“Understanding Professor Janda’s background and training allows one to better appreciate his contribution. His disability (polio-stricken), which began during his teenage years, enhanced his observational skills to almost unbelievable proportions. Because he was initially trained as a neurologist who later specialized in manual medicine and rehabilitation, he was uniquely qualified to explain the complex nature of chronic pain syndromes in a manner that integrated neurologically based principles with manual techniques.
Patterns of muscular imbalances led to stereotypically altered postures; altered gaits; trigger point patterns; joint dysfunctions; and pain syndromes. He found this movement was neurologically mediated and required a comprehensive understanding of manual techniques, such as manipulation and muscle-balancing measures, and neurophysiologically based techniques.” From Dr. Craig Morris’s Enduring Message of Vladimir Janda, MD, DSc, found in the April 12, 2003 issue of Dynamic Chiropractic
One of the most brilliant minds in the field of musculoskeletal rehabilitation was Vladimir Janda (pronounced Yonda). Although he passed away in 2002 in his mid-60’s, Janda’s legacy continues to grow. Listen to what a group of researchers wrote about him in a 2006 tribute in the journal Spine.
“An accomplished neurologist, he founded the rehabilitation department at Charles University Hospital in Prague, Czechoslovakia. He was one of the seminal members of the Prague school of manual medicine and rehabilitation that expanded its influence throughout Central and Eastern Europe. His observations regarding muscle imbalances, faulty posture and gait, and their association with chronic pain syndromes, etiologically, diagnostically, and therapeutically, influenced the rehabilitation world.”
Of all the MUSCLE IMBALANCE PATTERNS he discovered, the two biggest were unarguably the Upper and Lower Crossed Syndromes. Today we will be touching on the Lower Crossed Syndrome (I say “touching” because this is complex material about which volumes have been written).
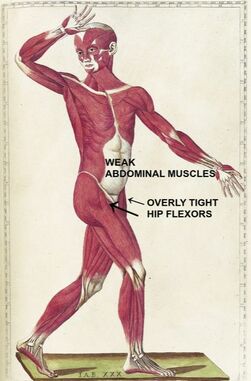
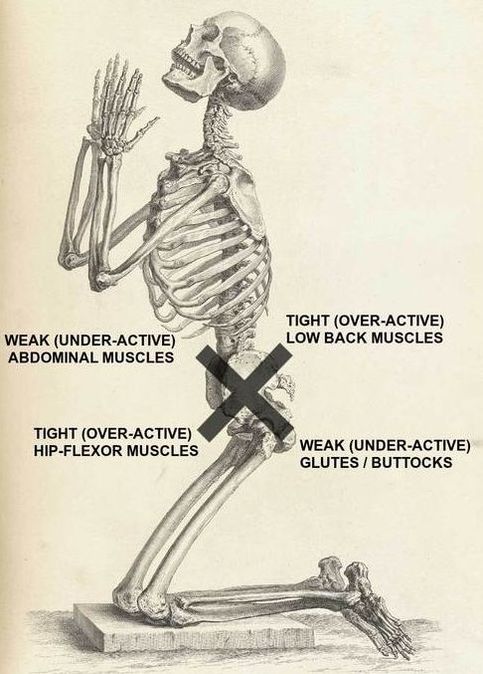
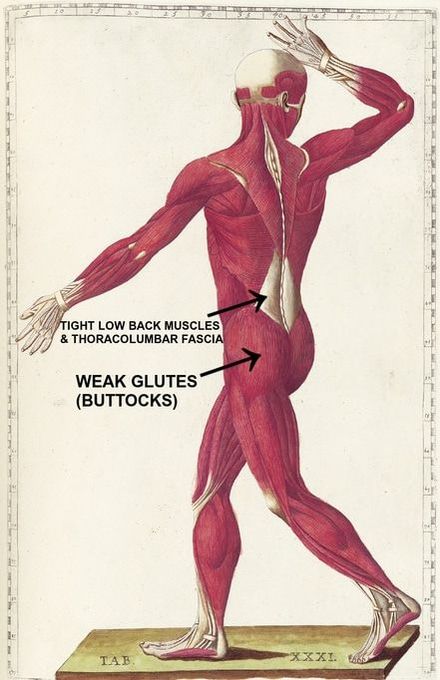
If you look at the pics at the top of the page (particularly the kneeling skeleton), you’ll notice that the pattern of Lower Crossed Syndrome takes the shape of an “X” — overly-tight HIP FLEXORS and THORACOLUMBAR MUSCULATURE, with weak BUTTOCKS and ABDOMINAL MUSCLES. What does this do? It creates massive amounts of mechanical stress in the low back that can be clearly seen in these side-by-side TEN SECOND VIDEOS of Adhesed Thoracolumbar Fascia as well as in the DEGENERATIVE CHANGES that follow.
It also sets people up for CHRONIC SACROILLIAC PROBLEMS or even issues of the hip rotator cuff (particularly the PIRIFORMIS MUSCLE). Beyond that, it contributes to a weak core (remember that the core is not simply your superficial abdominal muscles). While this is all great to know, the real questions are what does it look like clinically, what caused it in the first place, and what can you do to address it? Let’s look at these questions one at a time.
WHAT CAUSES LOWER CROSSED SYNDROME?
- Lower Crossed Syndrome Caused by Inactivity: Unfortunately, in our modern electronic society, this problem is not getting better. As you’ll see shortly, not only is activity critical for preventing or reversing Lower Crossed Syndrome, but it needs to be the proper sort of activity. Repeating the wrong sorts of movements over and over again can sometimes be as bad as inactivity. Sort of like repeatedly trying to drive a bent nail — you straighten it out but every time you hit it, it bends again.
- Lower Crossed Syndrome Caused by Inactivity: While sometimes this is a chicken and egg sort of thing (for instance, some people have genetic predispositions toward things like ‘sway back’ or horrendously pronated / supinated ankles) mostly it’s laziness and lack of effort. I spend a lot of time telling young people that their POOR POSTURE will end up haunting them as they get older. Are they listening? Some do and some don’t.
- Lower Crossed Syndrome Caused by Too Much Sitting: This is not surprising considering the insane amount of research that’s come out in the past decades on the detriments of sitting. Sick around and I’ll show you some simple remedies for this that you can do throughout the day (for instance, ‘The Founder’). Sitting is another reason that EXTENSION THERAPY can be such a huge benefit.
- Lower Crossed Syndrome Caused by Sports and Overtraining: I already see the indignation on some people’s faces and hear it in their voices. How in the world can sports (lots and lots of activity) cause problems if too little activity is one of the reasons people get Lower Crossed Syndrome? By their very nature, most sports tend to be very repetitive, as are their training regimens. GET INTO A RUT and you essentially spend all your time straightening and re-driving the bent nail I talked about in the first bullet — over and over and over again. This is why poor technique and imbalanced training (for instance, neglecting core strength or doing THE WRONG KIND of training) bends the nail even further, making it impossible to ever drive it into the board. It may look OK on the surface, but for all intents and purposes, it’s not functional.
- Others: There are certainly others so just remember that this list is not exhaustive.
WHAT DOES LOWER CROSSED SYNDROME LOOK LIKE?
WHAT IS THE CLINICAL PRESENTATION OF LOWER CROSSED SYNDROME?
I recall a football player while I was in college who, although he was absolutely ripped to shreds and big as a proverbial house, had incredible sway-back and a pooched stomach. He wasn’t overweight mind you — there was barely an ounce of fat to be found on this guy anywhere. But his belly looked like he was purposefully sticking it out.
LOWER CROSSED SYNDROME AND THE POOCHED BELLY:
While in this day and age it’s not uncommon to see a pooched belly because of BELLY FAT, I am not talking about belly fat here. Not that OBESITY can’t make this and other issues more difficult to see. Once you know what to look for when looking for lower crossed syndrome, spotting the “pooched belly” feature is easy.
LOWER CROSSED SYNDROME AND SWAY BACK (LORDOSIS):
This is having the extra amount of front-to-back curvature of the lumbar spine as seen in the lateral / profile view. The September 2011 issue of the European Spine Journal (Sagittal Spino-Pelvic Alignment in Chronic Low Back Pain) said, “Sagittal spino-pelvic alignment was different between patients with chronic low back pain and controls, suggesting the relationship between this specific pattern and the presence of chronic low back pain.”
Exactly three years to the month prior to that, the journal Spine (Classification of Sagittal Thoraco-Lumbo-Pelvic Alignment of the Adolescent Spine in Standing and its Relationship to Low Back Pain) compared lateral photographs of children to lateral X-rays of adults, concluding that, “Those adolescents classified as having non-neutral postures when compared with those classified as having a neutral posture demonstrated higher odds for all measures of back pain.”
In other words, POSTURE really is a big deal when it comes to chronic low back pain (or CHRONIC PAIN in general), especially if lower crossed syndrome is involved.
LOWER CROSSED SYNDROME AND THE ANTERIORLY TILTED PELVIS:
With overly tight hip flexors pulling down, and the overly tight low back pulling largely in an upward direction, the pelvis will typically tilt as seen by the curved arrow in the pelvis of the pic above left. Sometimes this will cause hyperextended knees as well.
LOWER CROSSED SYNDROME AND LOW BACK PAIN:
Just be aware that this problem (LBP) is so common in our society that Lower Crossed Syndrome is not the only cause here, but one of many potentials. However, due to the amount of sitting we do and that fact that sitting has been shown to inhibit certain trunk muscles, while firing others in an almost spasmodic fashion, we can see where this is headed.
HOW CAN YOU GO ABOUT SOLVING LOWER CROSSED SYNDROME ON YOUR OWN?
This, folks, is where the rubber meets the road. Nothing in this post really matters if you can’t start addressing this issue on your own. Just be aware that prior to the exercises and stretches that will be necessary for you to take care of your Lower Crossed Syndrome, you may have to deal with structural problems first (not to mention UPPER CROSSED SYNDROME).
The two biggies here are SUBLUXATION (including FORWARD HEAD POSTURE) and FIBROSIS / SCAR TISSUE / DENSIFICATION. No matter what you choose to call these pathologies (yes, they are FUNCTIONAL PATHOLOGIES), it can be difficult to the point of impossible to remodel TETHERED TISSUE without first breaking it. Just click the links if you aren’t sure what I’m talking about.
- TREAT LOWER CROSSED SYNDROME AS A SYSTEMIC PROBLEM: Honestly, this is good advice for whatever ails you. If you will treat this problem as though it has a significant INFLAMMATORY COMPONENT (which it very well might), your odds of solving it — along with any number of OTHER ISSUES as an added bonus — skyrockets.
- LIFTING WEIGHTS IS AWESOME FOR LOWER CROSSED SYNDROME IF YOU DO IT CORRECTLY: I’ve been fascinated by big muscles and feats of strength since I was a skinny, ripped, Kansas farm boy. I’m a huge fan of squats, dead lifts (since I don’t compete, I prefer a hex or diamond-shaped bar), power cleans, and the like. I must admit, however, that several years ago I fell in love with KETTLEBELL SWINGS. The thing about lifting weights is that if you are going to do it (and I think you should), you need to do it properly and with good form. This is waaaaaay more important than simply worrying about how much weight you are pushing. In the immortal words of David Carradine’s Kung Fu character, “Learn balance young grasshopper“.
- MAKE SURE YOU ADD FUNCTIONAL STRENGTH TRAINING TO YOUR POWER REGIMEN: As you just saw, I’m a huge fan of lifting weights. While POWERLIFTING is great fun, make sure that you are doing some FUNCTIONAL STRENGTH TRAINING AS WELL. There are so many videos on Functional Strength Training on YouTube I’m not even sure where to start. Another post for another day.
- TAKE CARE OF YOUR CORE: While this sort of goes hand in hand with the previous bullet, I have plenty of information specifically on TAKING CARE OF THE CORE, as well as including some basic stretches / yoga poses in a slide show below. I also included a neat little exercise I have been doing for about five years now called “The Founder”.
- REALIZE THAT IT IS POSSIBLE TO HAVE OTHER ABERRANT PATTERNS OF MUSCLE IMBALANCE: If you have crazy high arches like mine, you may very well tend toward tight glutes instead of flabby or weak glutes. The thing to remember about the body is that while you want to be aware of the most common patterns, also realize that it can get messed up in any number of ways for any number of reasons
- STUDY AND LEARN: Back in the dark ages (prior to the internet), finding quality information was tough. Now it’s easy. The cool thing is that there are a ton of YouTube Videos and websites full of exercise and stretching protocols. In all honesty, most of it really isn’t hard — it’s just a matter of CREATING A PLAN, starting small, and sticking with it. Having been to a number of seminars on Lower Crossed Syndrome (I was just at one a couple months ago), I can tell you that you can’t learn it all in a day. Read, watch videos, and learn. It’s just one more tool in your box for solving CHRONIC LOW BACK PAIN.
