
LOW TESTOSTERONE? UNDERSTANDING ITS MANY POTENTIAL CAUSES CAN HELP LEAD TO LONG LASTING SOLUTIONS

“Commercials don’t mention a 2009 study in the New England Journal of Medicine wherein a group of men on testosterone replacement therapy had more than four times the number of cardiovascular problems — so many that the study had to be halted. They also don’t make clear how risky exposure to testosterone gel is for others — female partners, children, even pets. The gel is actually notorious for transferring to others.
It can cause excess hair to grow on women’s faces and arms, deepen their voices, interrupt menstruation, and make them anxious and irritable. In children, exposure to testosterone gels and creams can cause premature puberty and aggression. And in pets, it can cause aggressive behavior and enlargement of the genitalia.” From John-Manuel Andoite’s article in the Atlantic called Should the Modern Man Be Taking Testosterone?
“Consumer advocate Dr Sidney Wolfe of Public Citizen says testosterone prescriptions in the US are 17 times higher per population than in the UK overall. And alarmingly, a fifth of those were for the non specific symptom of ‘fatigue’ and up to 9% were for men who had normal or high levels already. Some are given prescriptions without even having their levels checked. In 2014, Public Citizen actually filed a petition with the US Food and Drug Administration (FDA) requesting a strong health warning on all drugs containing testosterone.” From Ann Robinson’s article in The Guardian, Testosterone Therapy: Hope or Hype?
If you are a male, testosterone is awesome stuff. Exposure to the two month old fetus helps form the male sex organs. At puberty, production explodes, causing growth and maturation of said sex organs, along with secondary male characteristics such as deepened voice, body hair, beard, etc. Testosterone is part of what helps provide the male with self-esteem and their naturally-competitive nature.
It builds lean body mass (muscle), while increasing BMR (Basal Metabolic Rate) and preventing the deposition of fat. It’s also important for the formation of RBC’s (red blood cells). A “normal” amount should be above 300ng/dL (nanograms per deciliter), with an average of 7 mg being produced by the testes each day. I put the word normal in quotes simply because depending on one’s age, the range is 300 to 1,100 — a crazy amount of variation on what’s considered “normal” (550 is considered the average “functional” value).
The latest research says that about 25% of our adult male population has LOW TESTOSTERONE, with more of them obviously coming as they get older. However, due to any number of factors — many of which we will discuss today — there is a growing segment of the young adult male population who is dealing with Low T as well — an issue that is intimately tied to the precipitous decline in sperm counts of the males in Westernized countries (HERE).
The problem is that in similar fashion to what we discussed when we talked about the male menopause known as ANDROPAUSE is that an entire industry has grown up around diagnosing and treating low testosterone; most of it having to do with male HRT — Hormone Replacement Therapy — in the form of supplemental prescription testosterone. While this is certainly a viable option in some cases (emphasis on “some”), it should always be the last option. Why? Follow along as I show you. As a side note; if this problem pertains to you, even if you are young, make sure to read the post on Andropause.
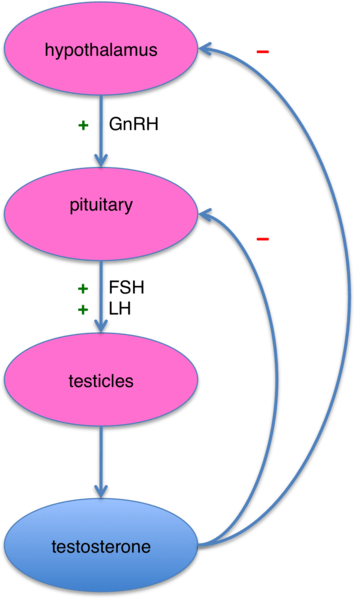
When you take exogenous testosterone, your body senses the high levels and in similar fashion to a thermostat, shuts down endogenous production (testosterone made by your own testicles) even further.
This is why, among numerous other health issues, the longer you are on supplemental testosterone, the more atrophy of your own testicles, and the greater the problem of ever getting your own production restarted and on track (bodybuilders and athletes using testosterone as a PED will often use the female hormone HCG (an LH analog) followed by a drug used to treat infertility in women, in order to try and restart endogenous production — stick with me and you’ll soon understand why they do this.
I would never say there is not a time or place to replace hormones (HERE is my article on female HRT and menopause), but it’s rarely the best case, and should never be done without doing things to deal with underlying causes. Otherwise, you run the risk of saturating hormone receptors and causing hormone “resistance” (think INSULIN RESISTANCE here, although there are several genetic forms of Testosterone Resistance such as Androgen Resistance and Androgen Insensitivity Syndrome).
In other words, the natural progression — particularly if you are young — is that it takes more and more of the hormone to get the same result, eventually hitting the point where there is diminished hormone function.
TESTOSTERONE PRODUCTION DIAGRAMS
According to Wikipedia, Hypogonadism, in terms of males, is defined as…
Diminished functional activity of the gonads / testes that may result in diminished sex hormone biosynthesis. Low androgen (testosterone) levels are referred to as hypoandrogenism. Other hormones produced by the gonads that hypogonadism can decrease include progesterone, DHEA, anti-Müllerian hormone, activin, and inhibin. Spermatogenesis may be impaired by hypogonadism, which, depending on the degree of severity, may result in partial or complete infertility.
Not only can Hypogonadism cause INFERTILITY, but not surprisingly it can cause SEXUAL DYSFUNCTION as well. But I am getting ahead of myself. If you really want to understand what causes Low Testosterone levels — particularly in the younger crowd — as well as grasp the differences between primary and secondary hypogonadism, you are going to have to understand a bit of neurology / endocrinology.
Hang in there, however, because it’s not as bad as it sounds. Understanding is important because a failure to grasp the basics of the following diagrams is probably a deal-breaker as far as understanding and solving your Low T issue is concerned. Let’s start with cholesterol.
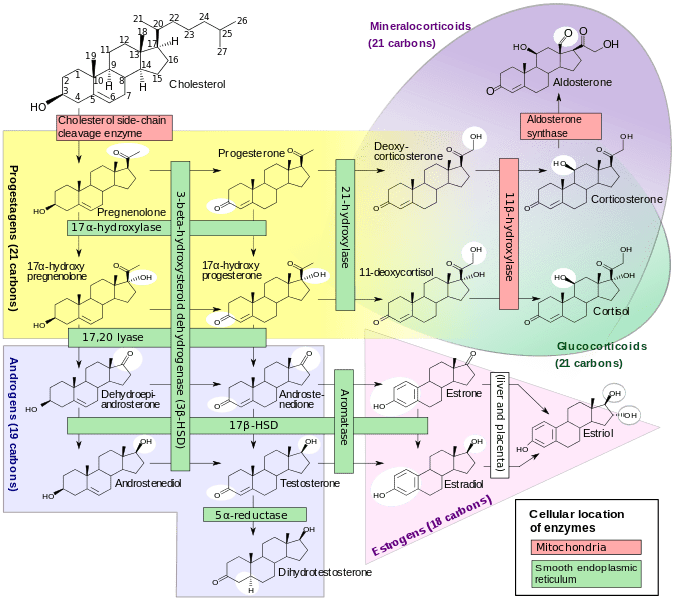
Why are CHOLESTEROL and Vitamin D so important as far as sex hormones are concerned — in this case testosterone? Namely because both testosterone and vitamin D are synthesized from cholesterol via an important intermediate called pregnenolone (remember pregnenolone because it will come up again momentarily).
The brilliant Chris Masterjohn puts it this way. “Since cholesterol is a precursor to vitamin D, inhibiting the synthesis of cholesterol will also inhibit the synthesis of vitamin D. Since sunlight is required to turn cholesterol into vitamin D, avoiding the sun will likewise undermine our ability to synthesize vitamin D. And since vitamin D-rich foods are also rich in cholesterol, low-cholesterol diets are inherently deficient in vitamin D.” But the importance of cholesterol does not stop there.
The flow chart diagram below not only shows (along with the proper enzymes) how cholesterol also happens to be converted into testosterone, but into estrogen as well (by the aromatase enzyme). What does all this really mean?
It means that even though numerous studies have shown that too much cholesterol (high cholesterol) has a negative impact on sex hormones, not surprisingly, so does low cholesterol, which is increasingly possible with our INDUSTRY-DRIVEN GUIDELINES on what should be considered normal. Interestingly, there are studies showing that supplemental testosterone increases cholesterol levels (this is one of its major potential side effects), while other studies show that it normalizes low testosterone.
For instance, a study from April’s issue of Sexual Medicine Reviews (Testosterone Replacement Therapy and Components of the Metabolic Syndrome) concluded that there is indeed, “a plethora of contrasting literature on the efficacy and safety of testosterone replacement therapy…. [which has] the potential to alleviate some of the morbidity associated with hypogonadism and Metabolic Syndrome.” What exactly is CARDIOMETABOLIC SYNDROME (aka pre-diabetes)? Just click the link.
However, seventeen authors writing in the February issue of EndoText (The Effect of Endocrine Disorders on Lipids and Lipoproteins) clarified this dichotomy by saying,
“Men with low testosterone levels may have high LDL cholesterol and triglyceride levels and decreased HDL cholesterol levels, although this relationship is confounded by obesity and the metabolic syndrome, a common cause of male hypogonadism. Androgen deprivation therapy results in an increase in LDL cholesterol, triglycerides, and Lp(a) and a decrease in HDL cholesterol. The effect of testosterone replacement therapy on plasma lipids and lipoproteins is modest and variable but high dose androgen therapy used by athletes can markedly decrease HDL cholesterol and also reduce Lp(a) levels.”
In essence, supplemental testosterone is more likely than not to foul up cholesterol levels; and while it might provide a “modest” improvement, the higher the dose (think steroids here) the more screwed up the lipid / cholesterol profiles are likely to be. Think this isn’t a big deal? Let’s briefly look at some studies.
Just a few months ago the Journal of Endocrinological Investigation (Influence of Vitamin D Levels on the Cardiovascular Profile of Hypogonadal Men) concluded that, “Our work shows the influence of vitamin D on cardiovascular profile in male hypogonadism. This effect seems to be more relevant in non-diabetic subjects. If these data were to be confirmed, vitamin D assessment might become mandatory in the clinical evaluation of cardiovascular profile in male hypogonadism.”
Back in Y2K, a study published in Metabolism (Effects of Simvastatin and Pravastatin on Gonadal Function in Male Hypercholesterolemic Patients) speculated that, “Inhibition of cholesterol biosynthesis by hydroxymethyl glutaryl coenzyme A (HMG-CoA) reductase inhibitors could, in theory, adversely affect male gonadal function because cholesterol is a precursor of steroid hormones.” A study published earlier this year in Endocrine Practice confirmed this when they concluded, “Long-term simvastatin intake reduces serum testosterone, estradiol, and progesterone levels in male rats.”
And just last month the Journal of Sexual Medicine published a study (Low Plasma Testosterone Is Associated With Elevated Cardiovascular Disease Biomarkers) that concluded, “Men with low plasma T levels exhibit increases in cardiovascuar risk markers, consistent with a potential increased risk of cardiovascualr disease.” While this is certainly not a shocker, what if I told you that this issue is potentially related to AUTISM?
Just two short months ago, the journal Autism Research published a study called The Role of Cholesterol Metabolism and Various Steroid Abnormalities in Autism Spectrum Disorders: A Hypothesis Paper in which they concluded (cherry picked),
“Testosterone is a steroid hormone which is directly metabolized from cholesterol. Based on evidence from the relevant research literature, we present a hypothesis that there may be a link between cholesterol, cortisol, testosterone, estrogens, progesterone, and vitamin D in autism spectrum disorder (ASD). ASD is diagnosed much more often in boys than in girls and there has long been speculation and controversy about the role of “the male brain” and sex hormones (particularly testosterone) in the pathogenetic chain of events leading to the clinical disorder and to “autistic traits”.“
I could go on and on here (including THESE STUDIES on statins and sexual dysfunction / infertility) but I realize that time is running short. Even though I wrote the article in the link above over three years ago, realize that it was late last year that the Journal of Clinical Lipidology (The Effects of Statin Treatment on Adrenal and Sexual Function and Nitric Oxide Levels in Hypercholesterolemic Male Patients Treated with a Statin) concluded that, “Erectile dysfunction complaints among men treated with a statin are not uncommon.”
Bottom line, while statin drugs certainly help lower cholesterol levels, they do nothing to deal with helping the body return to HOMEOSTASIS.
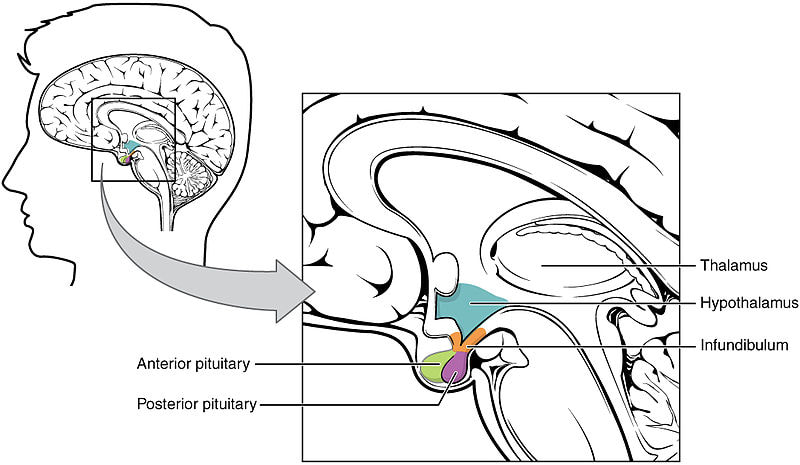
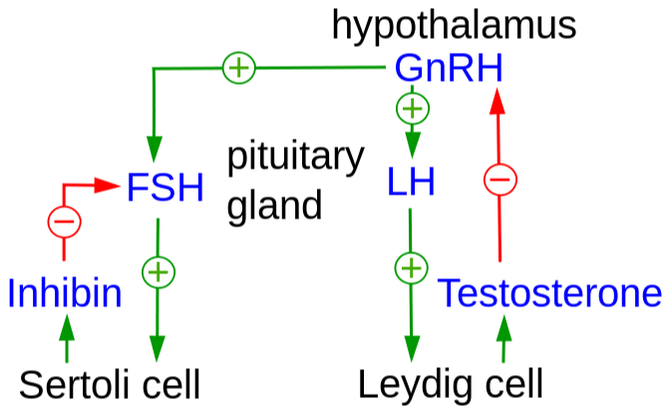
Some have referred to the production of sex hormones as more complicated than a “RUBE GOLDBERG CONTRAPTION“. Hopefully these diagrams above, along with this short explanation, will help simplify things. Gonadotropin-releasing hormone (GnRH) is exactly what it sounds like — a hormone that causes the release of the gonadotropins — follicle-stimulating hormone (FSH) and luteinizing hormone (LH) — from the anterior pituitary.
FSH stimulates Sertoli Cells in the testicles to produce sperm, and LH stimulates Leydig Cells in the testicles to produce testosterone. As you can see from the arrows and the + symbols (upregulation) or – symbols (downregulation), in a perfect world; if your body senses Low T it simply tells the hypothalamus to release more GnRH, which starts the process over again until testosterone levels are high enough.
The testosterone enters the body in it’s “free” state, but is quickly bound — or about 98% is bound, either by either Sex Hormone Binding Globulin (SHBG — about 60%) or albumin; about 38%. Because the bond that holds albumin to testosterone is much weaker that that between testosterone and SHBG, it is sometimes considered an easier-accessed form testosterone).
In order for testosterone to be used by the body, it must become unbound again or free, and after this it must hook up with testosterone receptors. Thus, in similar fashion to insulin, we want good sensitivity (as opposed to “resistance” —- INSULIN RESISTANCE). Men who use copious amounts of exogenous testosterone (i.e. STEROID USERS) can develop “Testosterone Resistance” in much the same manner.
Simple, isn’t it? It is until things start to go haywire. And when things go haywire, men end up with Low T. As you may be starting to realize, there are lot of ways to get there from here. What I want to do is cover a few of them in relationship to the diagrams we just looked at. In order to do that we are going to go right down the line and look at what happens when the points we just discussed go awry. For instance….
- Issues with cholesterol and vitamin d conversions as discussed earlier.
- If LH is high and testosterone is low, it is likely a testicular issue. This could come in many forms including nutrient deficiencies, mitochondrial dysfunctions, excess ROS (Reactive Oxidative Species), toxicity (either via exposure itself of by an inability to biotransform / detox), etc. We’ll talk about all of these in a bit.
- If LH is low and testosterone is low, it is pituitary suppression, often caused by immune dysregulation (rampant SYSTEMIC INFLAMMATION or neuroinflammation) due to head injuries, lippopolysachrides (LPS), HPA stress responses such as ADRENAL FATIGUE / SYMPATHETIC DOMINANCE, toxicity, etc).
- If testosterone is low, and either estradiol and/or DHT is elevated (DHT or Dihydrotestosterone is a significantly more potent form of testosterone that is found at levels between 1/10th and 1/ 20th of testosterone), it is a conversion issue.
- If free testosterone is low, and total is normal, it’s likely an issue with SHBG.
SIGNS THAT YOUR TESTOSTERONE
LEVELS MIGHT NOT BE UP TO SNUFF
When I woke up this morning I was feeling mighty good…. I woke up with wood. ZZ Top from 1985’s Afterburner (Woke Up With Wood)
My get up and go, just got up and went. Aerosmith from 1975’s Toys in the Attic (Sweet Emotion)
Why is knowing what low testosterone looks like such a big deal? Take a look at the conclusions of this ten year old study from the Journal of Clinical Endocrinology and Metabolism (Decline in Male Testosterone and Sex Hormone Binding Globulin Serum Levels in Danish Population Surveys).
Revealing something that others have shown as well, the authors concluded that testosterone levels have dropped precipitously over the past decades. “In addition to this expected age effect [older dudes having less testosterone than younger dudes], significant trends in testosterone and SHBG serum levels were observed in age-matched men with lower levels in the more recently born/studied men.“
As crazy as it might actually seem, there is a group of physicians led by Dr. Malcom Caruthers, a professor in the Alzheimer’s and Aging Department of Edith Cowan Unversity in Australia, as well as President of the Society for the Study of Androgen Deficiency (the Andropause Society), who believe that the amount of testosterone is not the issue as much as one’s level of resistance or sensitivity to the hormone.
Thinking of testosterone in terms of insulin, this makes sense. No one wants massive levels of insulin in their bloodstream as this leads to all sorts of problems (including receptor saturation and subsequent resistance). Instead, they want low amounts of insulin, with a high degree of receptor-sensitivity to it. More on this topic later, but for now, let’s look at some of the causes / symptoms of Low T (these are in no particular order).
- LOW TESTOSTERONE; GENETICS: Although the EPIGENETICS -vs- GENETICS debate has taught us that genetics get far more credit for sickness and disease than they should, there are some genetic conditions that definitely predispose one to Low T. Some of these include Down’s Syndrome, Kallmann’s Syndrome, Prader-Willi Syndrome, Klinefelter’s Syndrome (not only do I have a few patients with this, I have read that incidence is growing exponentially), Hemochromatosis (too much iron), Myotonic Dystrophy, Sickle Cell Anemia, and any number of others. Bear in mind that for the most part, these are rare and/or obvious.
- LOW TESTOSTERONE; BLOOD SUGAR DYSREGULATION AND/OR OVERWEIGHT / OBESITY: This, folks, is the low-hanging fruit, and can essentially be boiled down to INFLAMMATION (sugar and carbs that break down rapidly to sugar are some of the most inflammatory things you can put in your mouth — HERE), and is unarguably the number one reason guys end up with Low T, young or old. Whether you are OBESE (particularly if you have A BIG BELLY), a CARB JUNKIE, suffer from cardiometabolic syndrome (PRE-DIABETES), DIABETES, or insulin resistance, they are all different sides of the same dice. As there are literally hundreds of studies on this point, I’ll not not belabor it. BTW, this is the easiest cause of Low T to fix.
- LOW TESTOSTERONE; YOU HAVE A HISTORY OF TBI / MTBI OR HARDCORE WHIPLASH: TBI AND MTBI can cause so many problems it will literally make your head swim (literally — VERTIGO). If you have a problem in either your HYPOTHALAMUS or your PITUITARY, it doesn’t matter if your testicles are triple turbo charged, they won’t be able to make testosterone, or at least make the quantities needed for you to function properly and feel good. This is where an evaluation by a FUNCTIONAL NEUROLOGIST (not necessarily a medical neurologist) can make a huge difference. In case you think this is a minor point, listen to some of the conclusions found in a 12 year old issue of Clinical & Translational Endocrinology (Hypopituitarism After Traumatic Brain Injury). “Traumatic brain injury (TBI) is one of the main causes of death and disability in young adults, with consequences ranging from physical disabilities to long-term cognitive, behavioural, psychological and social defects. Post-traumatic hypopituitarism was recognized more than 80 years ago, but was thought to be a rare occurrence. Recently, TBI has been demonstrated to be a frequent cause of hypothalamic–pituitary function impairment, contributing to a delayed or hampered recovery in many TBI patients. A high incidence of sex-steroid deficiency has been reported in the immediate post-TBI period. In this phase, testosterone concentration has been shown to negatively correlate with the severity of injury. Testosterone levels in men and estrogen levels in women significantly fall within 24h following brain injury and remain lowered for 7–10 days. Testosterone levels may return to normal after 3–6 months or remain low.” In case this didn’t sink in the first time, read it again; especially if you’ve ever hit your head hard or had a WHIPLASH of some sort.
- LOW TESTOSTERONE; HPA AXIS DYSREGULATION: As you just saw in the bullet point above, a properly-functioning HPA (Hypothalamus / Pituitary / Adrenal) Axis is critical for hormone regulation. If you are one of those people who is massively stressed out (mentally, emotionally, dietarily, or due to chronic illnesses / chronic infections) it is not only likely that you are living in a state of SYMPATHETIC DOMINANCE and ADRENAL FATIGUE that will suck the life right out of you, you may be seeing the consequences of a pregnenolone steal. Because all of your steroid hormones come from pregnenolone via cholesterol, stress will cause huge amounts of pregnenolone to be shunted to CORTISOL production instead of sex hormones via the DHEA (Dehydroepiandrosterone Sulfate) pathway (go back and look at the cholesterol flow chart diagram), and often characterized by low levels of DHEA. A Warning to those of you supplementing with pregnenolone — you may be making things worse by feeding the cortisol path (supplementing with DHEA can also be problematic for those with Adrenal Fatigue). Be aware that cortisol’s main job is to help raise blood sugar in response to stress, actually creating conditions whereby the body tends to becomes resistant to the effects of insulin as well as causing a loss of lean body mass as you start breaking down protein to create even more blood sugar via a process known as gluconeogenesis. The problem is that because you are probably not actually in a true “FIGHT OR FLIGHT” situation, this excess sugar is then stored as fat — usually as belly fat.
- LOW TESTOSTERONE; INCREASED BODY FAT: In light of what we’ve seen so far, it’s pretty easy to see how this happens with Low T. Just remember that estrogen — the female opposite of testosterone — is made not only in the ovaries, but in fat cells as well. It’s one of many reasons women are naturally designed to have more body fat than men. Go back to our cholesterol diagram and notice that if testosterone levels get too high, the body will start converting testosterone to estrogen via the aromatase enzyme —- a reason that fat men and guys who have used supplemental testosterone will sometimes develop man boobs (“moobs” — referred to in the bodybuilding community as “bitch tits” or by physicians as gynecomastia). Just remember that the thing that tends to drive this pathway most is being fat. The end product of this is that increased levels of female hormone in the male is going to cause some funky side effects, including excess fatty deposition in all the worst places. It’s why men on prescription testosterone must sometimes be given aromatase-blockers (breast cancer drugs). A two year old study from the American Journal of Men’s Health (High Estrogen in Men after Injectable Testosterone Therapy: The Low T Experience) put the number of men on T-therapy experiencing this phenomenon at 20%. Not only this, but the journal Reproductive Biology and Endocrinology stated back in 2011 that, “Long-term efficacy and safety of the use of aromatase inhibitors has not yet been established in males, however, and their routine use is therefore not yet recommended.“
- LOW TESTOSTERONE; LOSS OF MUSCLE MASS: It’s also not tough to see how Low T is going to cause not only an increase in body fat, but a loss of muscle mass as well. Another way to think about this is that athletes or bodybuilders who are trying to increase muscle mass and strength quickly, often times resort to various forms of artificial testosterone (anabolic steroids, not to be confused with corticosteroids such as cortisol or cortisone). This loss of lean body mass one of the chief reasons that men with Low T will frequently have BACK PAIN or joint pain.
- LOW TESTOSTERONE; LOW SEX DRIVE AND LACK OF MORNING ERECTIONS: Let me put it to you this way, if you are a guy, and you aren’t thinking about sex on a regular basis (science says we men think about it 20-35 times a day — not every seven seconds as has been widely reported) or waking up with wood, there’s something wrong. Is it necessarily due to Low T? No, but it’s a good place to start looking.
- LOW TESTOSTERONE; YOU STRUGGLE WITH ALL SORTS OF MENTAL ISSUES: This could mean anything from DEPRESSION, ANXIETY, and mood swings to stress (which we’ve already discussed at length), to a loss of motivation, loss of competitiveness, loss of stick-to-itiveness, or an inability to concentrate. If you want to look up the studies, feel free (Pubmed dot com). Yes, there are actually studies on the ability of Low T to leave men feeling unmotivated.
- LOW TESTOSTERONE; YOU HAVE NO ENERGY: For some of you, even if you had the motivation, you wouldn’t have enough energy to get er done anyway. In fact for some of you, it’s all you can do to get through the day without collapsing in a heap. While this can certainly be due to other factors including the HPA Axis issues discussed earlier, Low T can be a culprit as well.
- LOW TESTOSTERONE; YOU HAVE A LOW SPERM COUNT: Trying to get pregnant (in our modern era I will clarify by asking if you are trying to impregnate your wife)? With what we’ve already seen concerning falling rates of ‘normal’ testosterone, we shouldn’t be shocked that SPERM COUNTS are less than half of what they were just a few short decades ago. While there are certainly a number of reasons for this, Low T cannot be overlooked.
- LOW TESTOSTERONE; ARE YOU SLEEPING? A couple of summers ago the journal JAMDA (Sleep Duration and Disturbances Were Associated With Testosterone Level, Muscle Mass, and Muscle Strength….) looked at the sleeping habits of 1,300 older men and concluded that, “Testosterone increased with increasing sleep duration up to 9.9 hours.” Four years before that, JAMA Network published a study called Effect of One Week of Sleep Restriction on Testosterone Levels in Young Healthy Men, in which they concluded, “Daytime testosterone levels were decreased by 10% to 15% in this small convenience sample of young healthy men who underwent 1 week of sleep restriction to 5 hours per night, a condition experienced by at least 15% of the US working population. By comparison, normal aging is associated with a decrease of testosterone levels by 1% to 2% per year.” Unfortunately, if you have Low T you are much more likely to be fat — the very condition that causes SLEEP APNEA. A 2016 article by Kevin Asp (Low Testosterone and Sleep Apnea: Reasons, Risks, & Treatment) revealed that “Studies published in the Journal of Clinical Endocrinology show that men of all ages with low testosterone do not sleep well in general: they sleep less efficiently, enjoy less rapid-eye movement (REM) sleep and awaken more frequently. Untreated sleep apnea for anyone, at any age, can be held accountable for causing or contributing to many other known chronic health conditions, such as hypertension, depression, diabetes, obesity, stroke, and heart disease.” As you can see, poor sleep habits help contribute to the viscous cycle of everything we’ve been talking about today.
- LOW TESTOSTERONE; YOU HAVE THYROID PROBLEMS: Even though there are many more women struggling with THYROID PROBLEMS than there are men, there is a definite link between Thyroid function and the male’s ability to adequately produce testosterone. For starters, if you look at the symptoms of low thyroid function and Low T, they are for the most part, very similar. Secondly, peer-review has shown that hypothyroidism decreases free testosterone, increases prolactin (which decreases testosterone) as well as creating less than optimal LH responses to GnRH. There are numerous endocrinological studies concerning this relationship (for instance, see The Interrelationships Between Thyroid Dysfunction and Hypogonadism in Men and Boys in the journal Thyroid). “Primary hypothyroidism is associated with hypogonadotropic hypogonadism…” And it’s not like any of this is new information. Clear back in 1987, the American Journal of Medicine (Abnormal Testicular Function in Men with Primary Hypothyroidism) concluded that, “abnormalities of gonadal function are common in men with primary hypothyroidism.” There are dozens of studies attesting to this fact. Oh, and in case you were not aware, low thyroid function causes insulin resistance, which as you’ve already seen, is heavily associated with Low T as well.
- LOW TESTOSTERONE; YOU ARE TAKING DRUGS / MEDICATION OR CONSUMING ALCOHOL: Here’s the thing folks, drugs of all kinds tend to mess you up whether pushed or prescribed (HERE are a few of my posts attesting to this fact). Want to see a list of some of the drugs (as well as drug combinations) that are specifically associated with erectile dysfunction? Then check out THIS CRAZY POST I did three and a half years ago. I’ve already talked about the way that statins block cholesterol production — the source of all sex hormones — but when I think of sexual dysfunction associated with a drug, it has to be ANTIDEPRESSANTS. The problem is so bad that I’ve done two posts specifically devoted to it (HERE and HERE). There are some quite freaky studies linking anti-acne drugs to Low T as well. PPI’s (heartburn and acid refulx drugs) are notorious for this, not to mention the fact that there are numerous studies linking OPIOIDS to Low T (one study shows 5x lower). While we’re at it, just realize that there are ample studies linking heavy alcohol use to to Low T, with the worst offender by far being beer (numerous studies show that alcohol use in men tends to lower T while raising estrogen), probably due to the ESTROGENIC EFFECTS OF THE HOPS (this might be a great time to mention that unfortunately the ligans in flax seeds have a similar effect).
- LOW TESTOSTERONE; YOU HAVE ANEMIA: ANEMIA is a deal-breaker for most chronic conditions (seen far more commonly in women than men simply because they bleed monthly). Testosterone stimulates erythropoietin — the hormone that causes you to increase your production of RBC’s (red blood cells).
- LOW TESTOSTERONE; YOU HAVE GUT DYSFUNCTIONS: In case you missed it previously, just realize that if you have chronic GUT DYSFUNCTIONS such as DYSBIOSIS, ISSUES WITH INTESTINAL PERMEABILITY, or both, you are going to have some serious issues with your health. All health. Every area. Period. Huge amounts of inflammation begin in an unhealthy Gut, and this inflammation will affect brain function (HERE), including the hypothalamus and pituitary. Dysbiosis is one of those unique animals that jacks testosterone levels in women (PCOS), while tanking it in men (HERE). Believe me when I say that there is enough material in this bullet to write a book (I have a huge post on this relationship called ENDOGUT).
- LOW TESTOSTERONE; YOU HAVE SOME SORT OF CHRONIC INFECTIONS: While this could be a dysbiotic condition I discussed in the previous bullet, there are all sorts of chronic infections that people end up with that are known to affect their levels of testosterone. For instance, there are tons of studies linking HIV to Low T. But what’s far more common and insidious are things like CMV (Cytomegalo Virus), EBV (Epstien Barr Virus — both are very common infections that cause mono), tick-borne illnesses, and even PARASITES, the defining characteristic of which is lethargy and generally feeling like crap (HERE). All of these cause increased systemic inflammation (CRP), which in turn leads to Low T. The brilliant Ben Greenfield puts it this way in his article Blame the Bugs: How Stealth Pathogens Are Making You Fat, Tired, and Brain Dead. “Any type of inflammatory stressor will increase aromatase activity, the enzyme that converts testosterone to estrogen.“
- LOW TESTOSTERONE; YOU HAVE A DANGEROUS WORK ENVIRONMENT: There are about a million studies on ENDOCRINE DISRUPTORS of all sorts. If you are exposed to chemicals or artificial smells in your work environment, you may be screwing up your entire endocrine system (see my EndoGut link above), not just your ability to make testosterone. This is why BIOTRANSFORMATION (the official word for detoxification) is such a big deal in our modern age. If you have problems in your biotransformation pathways, you will have endocrine issues.
- LOW TESTOSTERONE; OTHERS: Look; my point here is not to write a definitive post on the subject. It’s simply to get you thinking, and to hopefully point you in the right direction to do your own research as Low T can be caused by such a wide variety of problems.
WHAT IT TAKES TO RAISE LOW TESTOSTERONE LEVELS WITHOUT RESORTING TO SUPPLEMENTAL TESTOSTERONE
There are enough articles and studies on what it takes to increase your testosterone levels that at the very best, it can be extremely confusing. The world wide web abounds with both information and sales pitches for their products — most of which are complete and total crap. Honestly, for most of you if you simply follow some basic health premises, you’ll see some great changes.
- LOW TESTOSTERONE; GET YOUR WEIGHT AND CARDIOMETABOLIC HEALTH IN ORDER: Poor cardiometabolic health is a double-edged sword. Numerous studies have shown that Low T is directly related to poor cardiometabolic biomarkers (BLOOD SUGAR, cholesterol which we already talked about, triglycerides, C-reactive protein, etc, etc), but that the inverse is true as well. This is why Low T is not only tied to you feeling like crap, but according to the Journal of Endocrinology and Metabolism (Endogenous Testosterone and Mortality in Men: A Systematic Review and Meta-Analysis) is actually “associated with increased risk of all-causes of death.” And even though we’ve talked about it several times already, remember also that increased body fat promotes increased activity of the aromatase enzyme. For the record, the optimal level of body fat for males is considered to be between 7-15%.
- LOW TESTOSTERONE; GET YOUR FATS FROM AND CARBS FROM GOOD SOURCES / EAT THE RIGHT STUFF AND AVOID EVERYTHING ELSE: Even though the American Heart Association is still promoting crappy oils like those made from corn or soy, thinking Americans know better (HERE). There are lots of studies showing that HEALTHY FATS are where it’s at, and that the afore-mentioned fats, along with TRANS FATS — are serious destroyers of men’s testosterone-producing abilities. BTW, I never met a SUGAR/CARB ADDICTED guy who did not eventually move into diminished testosterone production and increased cortisol production (once this starts to happen it’s typically a landslide). It’s why I promote this simple advice in my clinic — EAT MORE AND EXERCISE LESS. Just make sure you are basing your diet on WHOLE FOODS (HERE is why I love Paleo for just about everything).
- LOW TESTOSTERONE; EASE OFF ON THE CARDIO AND GET SERIOUS ABOUT STRENGTH TRAINING: Speaking of exercise….. Because time and time again, intense long-duration exercise (i.e. hardcore cardio) has been associated in peer-review with both LGS and increased cortisol production (Leaky Gut and Adrenal Fatigue) — problems almost universally found with any number of chronic conditions — my advice here is relatively simple. Focus on exercises that actually cause your body to boost testosterone production. RESISTANCE TRAINING, HIIT, etc. In most cases you can get done what you need to get done in a half hour or less. Make sure to incorporate some “POWER” movements or things like KETTLEBELL SWINGS. Just realize that if you are already in a state of severe chronic fatigue, this bullet could be the equivalent of you climbing in the hole and digging your own grave — especially if your job is physical.
- LOW TESTOSTERONE; REST, DE-STRESS, AND SLEEP: As you may have already guessed, this is a critical point. The adrenal hormone we talked about earlier, cortisol, is the number one antagonist of testosterone. Think about it this way; cortisol is not only catabolic (it promotes the breakdown of tissue, particularly lean body mass), it promotes belly fat, ESTROGEN DOMINANCE (yep, this can and does happen to men — when it comes to hormones, ratios rule), and insulin resistance, when exposed to the hormone regularly / constantly. There are dozens of “sleep hygiene” articles that can be found online. The bottom line is that you are going to have to figure out ways to get out from under the stress (much tougher if that stress is due to chronic infections — HERE and HERE are other examples of this phenomenon).
- LOW TESTOSTERONE; AVOID ENDOCRINE DISRUPTORS: Listen folks; the testicles as well as the hypothalmus and the pituitary are all part of the endocrine system. This means that you should avoid ENDOCRINE DISRUPTORS like the plague (HALOGENS as well). Dr. Vodjani’s Cyrex Labs actually makes blood tests to see if you are reacting immunologically against any number of these creatures (BPA, parabens, etc, etc).
- LOW TESTOSTERONE; LOW LEVEL LASER THERAPY (LLLT) AND ELECTRICAL MUSCLE STIMULATION: Seven Japanese researchers publishing in a 1993 issue of the European Journal of Applied Physiology and Occupational Physiology (Rapid Increase in the Number of Androgen Receptors Following Electrical Stimulation…) concluded exactly what the study’s title says. As a proponent of LLLT (LOW LEVEL LIGHT THERAPY) in the form of Cold or Class IV Lasers; knowing how they work (click the link) helps explain why there are a number of studies showing how treating the testicles with light can increase production of testosterone. If you want to look at the studies, simply Google ‘LLLT Testosterone’. I am also hearing about increasing numbers of health problems associated with exposure to light from the “blue” part of the spectrum. I must say that I absolutely love my LED lights, but am looking for blue filters (HERE is another example of what I am talking about). I should not be surprised at this considering TED CARRICK has been using rose-colored glasses to treat patients for decades.
- LOW TESTOSTERONE; GET OUT IN THE SUN: Cholesterol is converted to Vitamin D in the presence of sunshine, and good levels of Vitamin D positively correlate to testosterone levels. Listen to the conclusions of this 2010 study from the Journal of Endocrinology. “Men with sufficient D levels had significantly higher levels of testosterone and FAI (free androgen index) and significantly lower levels of SHBG when compared to D-insufficient and D-deficient men. In linear regression analyses adjusted for possible confounders, we found significant associations of D levels with testosterone, FAI and SHBG levels. D, testosterone and FAI levels followed a similar seasonal pattern with a nadir in March and peak levels in August.” Maybe it’s why I enjoy the CURRENT RIVER so much. Speaking of that cold Current River, there is also anecdotal evidence that keeping the jewels cool has the ability to increase T. The truth is that they are supposed to be a bit cooler, which is why they hang outside of the body.
- LOW TESTOSTERONE; GET OFF OF EVERY DRUG YOU CAN POSSIBLY GET OFF OF: Not only do numerous drugs have antibiotic effects that destroy Gut Health (HERE), which can affect all hormones, but as I showed you earlier, they screw up your testosterone levels as well.
- LOW TESTOSTERONE; WHAT ABOUT SEX ITSELF? Because our society is saturated in it, the first thing I want to do is talk about PORN ADDICTION. The Association for Natural Psychology puts it this way, “Pornography triggers certain hormones in our bodies, such as adrenaline, and stimulates the production of testosterone, oxytocin, dopamine, and serotonin. Indulging in pornography is like indulging in a chemical cocktail. It gets you going. Like any drug, though, once the “rush” is over, there is invariably a letdown. To get the rush again, you have to take another hit later. Therefore, the addiction potential for pornography is enormous.” What I find as interesting as anything are the number of men who are giving up porn that are not doing so for religious purposes (see link above). Want to see some of the studies on the topic? HERE, HERE, HERE, HERE, HERE, HERE, HERE, HERE, HERE, HERE, HERE, HERE and HERE. Although it would be difficult to come to hard and fast overall conclusions based on these and other studies, I would suggest that you read these studies in light of the first link in this bullet point.
- LOW TESTOSTERONE; OTHER: Here’s the thing; there is so much information out there on what you can do to increase testosterone levels, it can make your head swim. I saw a study saying “power poses” (postures of authority) had the ability to increase T by 20% in a matter of minutes. Unfortunately, this was one of THE MAJORITY OF MEDICAL STUDIES THAT CANNOT BE REPLICATED. You will also find a lot of weird or conflicting advice. For instance, there are numerous studies showing that both CIGARETTES and WEED actually increase testosterone levels (albeit with a wide array of other side-effects such as low sperm counts). Also be aware that there are numerous studies showing that low testosterone not only has lots of problems associated with it (see earlier list), but that by increasing these levels, you can effectively solve many of said problems. Never, forget, however, that there are many many studies that address the potentially devastating consequences of male HRT — not the least of which is its almost universal propensity to shut down endogenous testosterone production. If you are interested in seeing a general protocol for getting started taking your health back, make sure to take a quick peek at THIS POST. The supplements I recommend are protomorphegens / glandulars from Standard Process; Simplex M, and their Pituitary and Hypothalamus supports respectively (Simplex M has small amounts of both of these, along with their Thyroid formula).
Be aware that some of you might require work with a FUNCTIONAL MEDICINE SPECIALIST of some sort to get this thing sorted out. Also be aware that there are many many practitioners jumping on this bandwagon due to its popularity. In other words, watch out for “FUNCTIONAL MEDICINE LITE“. If you are liking what you are seeing on the site, be sure to spread the wealth by liking, sharing or following on FACEBOOK.
