
??? Primary or Secondary ???
If you look at my TRACK RECORD, you will soon realize that I am probably getting as good of results with the Conservative Management of people with Piriformis Syndrome as anyone, anywhere — period. But my goal is to see everyone get radically better — AND WHEN THEY DO NOT, it is very frustrating to everyone involved. Understanding some of the underlying causes / contributing factors of Piriformis Syndrome goes a long way toward understanding why it is such a complex and difficult problem to effectively treat in certain individuals.
PRIMARY PIRIFORMIS SYNDROME
I certainly do believe that Piriformis Syndrome can be a primary problem of the Piriformis Muscle —- particularly when a person has had severe trauma to their buttock region. One time I had a patient who was hit in the buttock by a front end loader. Another had a tree felled onto his rear end. Needless to say, these were classic Piriformis Syndromes that was directly related to the Piriformis Muscle itself. However, I think that in most cases of Piriformis Syndrome, the problem tends to be secondary. Allow me to explain.
Some of the more common underlying problems that can cause Piriformis Syndrome — or just make it difficult to fix, include:
- POOR FOOT OR LOWER EXTREMITY BIOMECHANICS: I have crazy high arches. I broke my right ankle three different times within a ten year period. This combination caused me to develop Chronic Pain not only in my foot, but in my right Piriformis Muscle as well (something that I still periodically battle if I do certain things). If you stand with your hands on your butt and then bow your knees outward like a cowboy, you will feel how tight the Piriformis Muscle gets. High arches drive you to the outsides of your feet, causing a “bow legged” position that can cause tremendous pressure on the Piriformis Muscle. Fallen arches throw you into a “knock kneed” position, which can cause pressure on the Piriformis Muscle as well, but are typically easier to deal with. If you have extremely high arches, contact me. I will put you in touch with the only person I am aware of who truly specializes in custom orthotics for people with high arches.
- A SHORT LEG: This can be either an anatomical short leg, or functional short leg. Anytime that you take someone who is in serious pain and start messing with heel lifts, you had better know what you are doing —– and do it very slowly and cautiously. I have seen miraculous results with this simple trick. I have also seen health care providers cause Piriformis Syndrome with heel lifts.
- PELVIS SUBLUXATION / DISTORTION: SUBLUXATION simply means that you have bones that are either out of alignment or not moving properly in relationship to each other. Interestingly enough, many of my Piriformis Syndrome patients that I treated for years chiropractically, would respond tremendously to Chiropractic Adjustments. But they never seemed to hold as long as I thought they should. If you go HERE and scroll down to the x-rays of three “normal” pelvises, you will notice some significant pelvic torque. Does this torque always cause Piriformis Syndrome and Sciatica? Certainly not. But it can cause both.
- TENDINOSIS / TENDINOPATHY: I have seen several cases of Piriformis Syndrome start with a PULLED GROIN. The mechanical stress can eventually caused TENDINOSIS that alters the gait. In one case, no one had ever as much as looked at the groin, even though he mentioned it repeatedly to different doctors, therapists, and chiropractors over a five year period. Sometimes these TENDINOPATHIES are either totally or mostly asymptomatic —- at least at first. And sometimes they can be so distant from the site of pain as to seem like the two could not possibly be related. HIP FLEXOR issues are commonly related to Piriformis Syndrome as well.
- FASCIAL ADHESIONS: Fascia is arguably the most pain-sensitive tissue in the body. Couple this with the fact that with the possible exception of the PLANTAR FASCIA, it does not show up on MRI (HERE), and you have a recipe for disaster. This is just one of many reasons that people can go through multiple MRI’s and CT Scans that do not “show anything” (FUNCTIONAL PROBLEMS -vs- PATHOLOGY). And in even greater measure than tendon problems above, FASCIAL ADHESIONS can be far-removed from the site of pain. This is one of the chief reasons that the most famous whiplash research team of our era concluded nearly two decades ago that whiplash injuries lead to a host of, “bizarre and seemingly unrelated symptoms (HERE).”
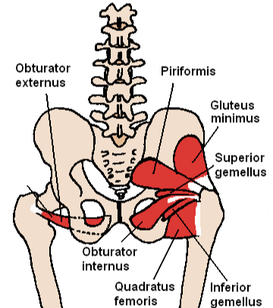
- DEEP FASCIAL ADHESIONS: A problem that can be particularly difficult to deal with is when a patient has FACIAL ADHESIONS that lie deep within the pelvis. If you look at pictures of the pelvic musculature below, you will notice that there are some muscles that are literally buried in the pelvis. This can make it all but impossible to access in a non-surgical fashion. And yes, all of these deep muscles are covered with Fascia in an almost identical fashion to the more superficial muscles. So, when you try and cut out the Piriformis Muscle, or surgically “Release” it, you end up with Scar Tissue — the very thing that may very well be causing your problem in the first place. Women who have had surgery for severe Endometriosis understand this concept better than anyone else.
- PIFIFORMIS SYNDROME DOES NOT SHOW UP ON ADVANCED IMAGING: Although I touched on this earlier, I will reiterate this point. Most of the people I see with hardcore Piriformis Syndrome have been through all sorts of diagnostic testing including advanced imaging techniques such as MRI & CT (HERE). In their minds, the pictures taken of their hind ends should “glow red” because of the severity of their pain. Instead….. nothing. I keep hearing about all sorts of new diagnostic techniques that are supposed to definitively show / prove the presence of Piriformis Syndrome. I am from Missouri — the “Show Me” State. Until someone proves to me that they are getting reproducible results with their diagnostics, I’m not buying it.
- ALL PIRIFORMIS SYNDROME IS NOT CREATED EQUALLY: I would like to tell you that all Piriformis Syndrome is the same. It’s not. I see Piriformis Syndromes that are intermittent and relatively mild. I also see Piriformis Syndromes that are severe — sometimes to the point where people are ready to end it all. Most people tend to fall somewhere in the middle. Although the less severe cases tend to respond instantaneously; the same thing can sometimes be said of the more severe cases. Without running my checks and actually treating a person, it is difficult for me to predict how well or how quickly a person is going to respond. The really nice thing about what I do is that we will at least have an idea whether or not I can help you after just one treatment. Although one treatment will certainly not “fix” your problem in its entirety; if it is going to change, you will see at least some degree of change within a few days.
- EXCESS WEIGHT: Although I have seen many extremely thin people with severe pain due to nerve entrapments such as Piriformis Syndrome, the fact remains that excess weight puts you at risk for almost any physical ailment imaginable — including Piriformis Syndrome. If you have Piriformis Syndrome and need to LOSE WEIGHT, get started today.
- POOR DIET / SMOKING: When I talk about diet here I am really talking about avoiding foods that are both Degenerative & INFLAMMATORY. And smoking is a no-brainer. When you smoke, you literally starve every cell, organ, and tissue in your body for OXYGEN. These are two things that are completely up to you. If you live with any sort of Chronic Pain and are still smoking cigarettes and eating a crappy diet, you have to knuckle down and remedy this situation if you want any hope of solving your problem!
- THE PAIN ITSELF: I have been telling people for years that CHRONIC PAIN does bad things to their brains. Recent research suggests that the brains of people with Chronic Pain atrophy at nearly 10 times the normal rate, becoming indistinguishable (on brain scans) from the brains of people with ALZHEIMER’S DISEASE or Dementia. And did you know that you can actually “learn” Chronic Pain? The more you shoot free throws, the better you get at it. Once you learn to ride a bike, you could not “forget” how to ride a bike if you wanted to. It all has to do with creating and developing nerve pathways. Unfortunately, the longer a person is in Chronic Pain, the greater chance of the pain being “imprinted” on a nerve pathway. There are ways to deal with this phenomenon, but it can be difficult for those who develop CLASS III CHRONIC PAIN.
- NARCOTICS USED TO TREAT THIS PAIN: Before I start, let me say that this is not a dig against people who have used pain meds. Although I never went down that road, I personally understand. If you have followed this blog, you are aware of the fact that a decade ago, I was ready to have my right foot amputated (thank God O didn’t). I know what Chronic Pain does to people (HERE), and the lengths that they will go to in order to get away from it. NARCOTICS are one way that people do this. The problem with this class of drugs is that what works to relieve pain today, will not work tomorrow —– repeat. And the science behind long term narcotic use has been proven to be fraudulent as well. But the real problem is the way that these opioids affect pain. When people who have spent a significant amount of time on opioids try to back off these drugs; or get off of them completely, they are often met with a shock. Their pain is worse than it ever was! Your body makes its own opiates, and when there are lots of opiates (drugs) already in your system, the body will shut down its own production. This is why it is so difficult to get off of these drugs — and why you may have incredibly heightened pain when you do come off.
- THE PROBLEM IS SYSTEMIC: What do I mean by this? Simply that I have seen people with Piriformis Syndrome (as well as ALL SORTS OF OTHER PROBLEMS) that is related to weakened or defective connective tissue. This might be some sort of AUTOIMMUNITY issue. It might be a genetic thing. It might be a METABOLIC DEFICIENCY OR NEUROLOGICAL PROBLEM. Or it might be some kind of poorly understood systemic disease process (HERE). Although I have successfully treated many cases of BILATERAL PIRIFORMIS SYNDROME, when I see bilateral problems or multiple site problems, the possibility that the problem could be systemic increases. Bottom line; if you have multiple sites of joint pain, tendinosis, or connective tissue dysfunctions, your problem could very well be SYSTEMIC. If this is the case, the first thing to do is to go about FIXING THE GUT. HERE is a great place to start researching this topic.
- THE PROBLEM MAY BE OF A SURGICAL NATURE: If you have followed this blog for any length of time, you are aware that I am not a big advocate of surgery. The truth is, study after study after study shows that huge numbers of surgeries of all sorts are unnecessary and do not change outcomes. In fact, many surgical procedures can leave people worse off. However, there is undoubtedly a time and a place for surgery. Although I would strongly recommend that you do everything in your power to avoid Piriformis Release Surgery, there are some brand new tests and procedures that may (might, could possibly, perhaps, perchance, etc) provide an answer for some of you hardcore suffers out there. I hope to be blogging on this topic in the fairly near future — probably sometime this summer.
PIRIFORMIS SYNDROME
MOSTLY A SECONDARY PROBLEM
Understanding this point is critical. Why so? Because in the same way that the medical community aims its treatment of OSGOOD SCHLATTER’S SYNDROME at the painful tibial tubercle (which is never the cause of this particular problem); in Piriformis Syndrome, most of the stretches, INJECTIONS, etc, are aimed at the Piriformis Muscle itself. Although this can bring about some temporary relief, it rarely brings about a complete resolution of the problem.
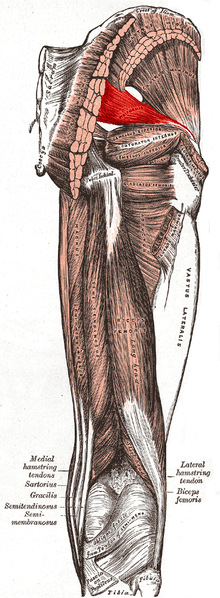
The two pictures below help to explain why the Piriformis Muscle can “pinch” or irritate the Sciatic Nerve — even though it is not actually the cause of the pinching. The Piriformis Muscle is the “where“. The “why” is the puzzle that has to be figured out and solved. It is my opinion that for many people, my clinic is a good place to start this process. Maybe my treatment protocols will help, maybe they won’t. But the bottom line is that you will know after a treatment. If what I do does not help, you can then take the next (more expensive and more invasive) step in the process.
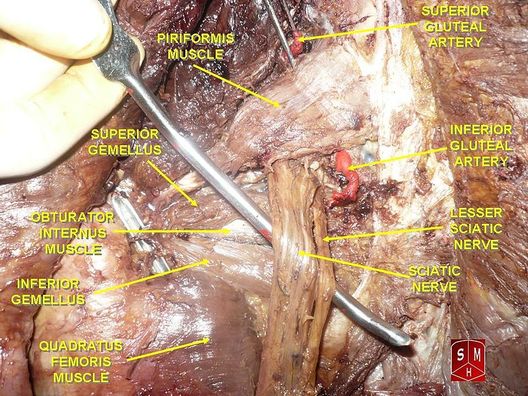
Image by Anatomist90
|
|
