
CHRONIC, NON-SPECIFIC BACK PAIN…
COULD THERE BE A SOLUTION FOR YOU?

The longer I’m in practice, the easier it is to see why so many people are not finding relief from or long-term solutions for their chronic pain. Particularly for their chronic neck or back pain.
- MEDICINE IS INCREASINGLY BASED ON TESTING: It’s inarguable that we’ve gotten away from TOUCHING PATIENTS or for the most part, even really examining them in any sort of meaningful way. For insurance companies to pay claims, there must be a “provable” diagnosis, with much of this “proof” coming in the form of imaging from CT, MRI, digital x-ray, etc, etc. There’s a problem with this approach….
- TESTS DON’T SHOW WHAT DOCTORS ARE LEADING PATIENTS TO BELIEVE THEY ARE SHOWING: When it comes to these tests, almost nothing is as it seems — or as patients are led to believe. There’s the fact that degenerative changes seen in the spine don’t correlate well to patient’s symptoms (HERE). There’s the fact that routine physical examinations are not catching simple orthopedic problems (i.e. diminished ranges of motion) prior to them becoming complicated and chronic (HERE). There’s the fact that at least 50% of the pain-free population is walking around with visibly herniated discs in their spines (HERE). And in all honestly, this bullet barely scratches the surface of how bad things really are in the realm of testing and treatment (HERE).
The world’s foremost leading expert on spinal discs and biomechanics, Dr Stuart McGill, says this on his website…….
“Back pain always has a cause. Most patients receive poor advice that remains a barrier to recovery. They stay in pain unnecessarily. Some receive pain-numbing medication that does not stop the cause of pain. Some are told that they must learn to live with the pain, rather than being shown why they have pain together with a roadmap of the steps to reduce it. The key to success is to understand the pain mechanism, and address the mechanism.”
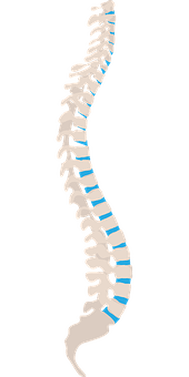
When looking at a lateral view of the spine, the first thing we notice is the curves. The (normal) forward curve in the neck and low back is known as “lordosis” or “lordotic,” while the mid-back curve runs the opposite way and is known as “kyphotic” or “kyphosis”. What do these curves do? For starters they allow normal movement, both segmentally and sectionally (HERE). Proper curves also create a spring-like function that allows the spine to act as a sort of shock absorber; particularly important if you work on CONCRETE or other hard surfaces. Without proper curves your spine would take a pounding of epic proportions. The curves work to distribute weight and force as well as transferring muscle energy to where it’s needed. As you might imagine from looking at the picture; when spinal mechanics are off, the end result is that there is abnormal distribution of forces to spinal discs — or maybe more accurately, to parts of the disc where said force should not be. Allow me to give you an example.
If you look at the low back of the picture above you will notice a significant (normal) lordoctic curve. This curve helps explain why it’s not only important to use your legs when bending and lifting, but to take the next step and consciously train yourself to maintain the normal lordotic curve through those activities (in other words, to bend forward while maintaining this curve). In the pic you will notice that the discs are “wedged” and that the open part of the wedge is in the front of the spine, and the closed part of the wedge is at the rear. Why is this important to understand? Mainly because discs always herniate backwards.
While discs will often herniate some degree laterally, they virtually always herniate backwards (posterior), meaning that herniated discs — mostly from the low back or neck — have the potential to be pushed or squeezed into the spinal cord or spinal nerve roots that come from the cord. What does this have to do with maintaining normal lordotic curves?
These normal curves put an axial pressure on the backs of the discs (as opposed to the fronts of the discs). As you can see from the picture above, this squeezes down on the posterior aspect of the disc, while opening up the anterior or front of the disc and pushing it forward. This natural “wedging” of these discs makes it extremely difficult for the disc’s jelly center (the nucleus pulposis) to herniate (because without a horrific trauma the disc will not herniate forward), and explains why you will sometimes see this spinal position referred to as “closed-packed”. However……
Imagine what would happen to the low back or neck if there were either no curves, or even worse, a REVERSE CURVE. Now, instead of the discs having the “open” portion of their wedge to the front, the open part of the disc faces the back. This is what happens to your lumbar spine if you bend forward and touch your toes. No big deal. That is, no big deal until you start loading the spine. Imagine, however, bending forward and lifting something, while not consciously maintaining the normal curve in your back.
Not only are you opening the disc in the back, but the heavier the object you are lifting (or the more overweight you are), the more pressure you are exerting on the front of the spinal column and discs, as opposed to them carrying this force on the posterior parts of the spinal column (the facet joints). This pressure literally squeezes the disc backwards like squeezing a tube of toothpaste. When there is too much force, or more likely, too many years of poor lifting mechanics, the ligamentous fibers of the disc (the annulus fibroses) that hold the jelly-like nucleus in place begin to separate and tear. The result is that you are now in a position where disc herniations are not only possible, but increasingly probable (HERE is a basic video of what this looks like).
Let’s add one more variable to this situation. Let’s do some situps. After all, everyone knows that situps are good for your back because strong abdominal muscles promote strong discs —don’t they? Enter Stuart McGill. Decades ago, McGill was the lone voice in the wilderness, warning that situps were not only not good for your back, but were arguably one of the single worst things you could do to your spine. His research has shown why situps are one of the best ways to cause spinal problems, including herniated discs (HERE).
In a recent interview with Dr. William Morgan (A Conversation with the Preeminent Lumbar Spine Researcher: Stuart McGill, PhD); after discussing overuse of spinal imaging, McGill made this statement concerning what’s arguably the single most common spinal finding on radiologist’s reports DJD or DDD (degenerative joint disease . degenerative disc disease). “When they [radiologists] use the term degenerative disc disease, I put that in the same category as nonspecific back pain. It’s a garbage term.” Interesting because that is essentially what I said in THIS 2012 POST.
In the PORTION OF THE VIDEO INTERVIEW titled Mechanics of Injury For Lumbar Disk Herniations and Extrusions, those of you suffering low back pain will find some interesting tidbits as far as what put you there, as well as pointing you in the right direction to a solution. The biggest disappointment concerning this video was that two of the chief drivers of chronic back and neck pain were not really addressed; the first being SYSTEMIC INFLAMMATION, the other being micoscopic fibrosis or adhesion of the FASCIA, or more specifically, the thoracolumbar fascia (HERE, HERE, HERE, HERE, HERE, HERE, HERE, HERE, or HERE) — a factor that increasing numbers of experts are saying is responsible for the majority (as much as 70%) of chronic back pain. I would argue that if you add these two modes of thinking to the knowledge and protocols created by McGill, your results will be better yet. Allow me to explain.
What do we know about back pain?
- We know that back pain is the world’s number one leading cause of disability (HERE).
- We know that back pain and disc herniations are both considered “inflammatory” (HERE or HERE).
- We know that back pain is associated with increased potential of developing chronic neurological disorders and diseases (HERE).
- We know that in our sit-too-much society, both LOWER CROSSED SYNDROME and UPPER CROSSED SYNDROME are epidemics that are dramatically increasing in both numbers and severity.
- We know that there is an intimate relationship between chronic pain, chronic illness, adhesed fascia, inflammation, and fibrosis / scar tissue (HERE, HERE, HERE or HERE).
- We know that SCIATICA is often caused by VERY SPECIFIC FASCIAL ADHESIONS as opposed to disc herniations.
- We know that adjustments are helpful for many cases of spine-related pain (HERE). We also know that in many cases, these same adjustments don’t hold very well (HERE).
Although I could have taken this list further, it helps explain why even though one cannot ignore the biomechanical aspects of back and neck pain, it’s critical to realize there are other factors at play; particularly the chemical factors we refer to as “INFLAMMATION” — a factor known to put people into a true CONUNDRUM.
If you are interested in shedding systemic inflammation and starting the process of RESOLVING YOUR BACK PAIN, be sure and take a look at THIS POST. It will at least provide a few ideas as far as creating your own personalized EXIT STRATEGY is concerned. Also, be sure to like, share or follow on FACEBOOK if you appreciated this post because it’s still a great way to reach the people you love and value most.
